

Physical activity has a positive effect on the function of the whole human body system. The influence of physical activity on the development of the respiratory system is still a matter for debate. Swimming is considered the sport with the most profound effect on the lungs.
AimThe first aim was to determine pulmonary function and to correlate it with anthropometric features of sportsmen, represented by land- and the water-based elite athletes comparing with their sedentary counterparts; the second aim was to examine whether the training factors (frequency and amount) influence pulmonary function in swimmers, when controlled for anthropometric features.
MethodsThirty-eight elite male swimmers were matched for age and sex with two hundred and seventy-one elite football players and one hundred controls who were not involved in any routine exercise. Lung volumes were recorded by Pulmonary Function test and analyzed statistically.
Results and conclusionSwimmers had statistically higher values of VC, FVC, FEV1 and FEV1/FVC when compared to both the football players and the controls, as the latter two showed no in-between differences. There was significant positive correlation between age, body weight and body height and each of the above named pulmonary parameters, when presented separately for swimmers, football players and the control group. When controlled for the anthropometric features, larger lung volumes in swimmers were not influenced by training period, age at the beginning of training and weekly extent of personal training. Further comprehensive longitudinal studies are needed to confirm these observations.
Better function of every system in the human body is achieved by regular exercise. Muscular strength in general (including respiratory muscles) is developed by systematic training, so it is assumed that it has a positive effect on the lung function. Recent studies have shown that athletes have larger capacity of the respiratory system when compared to their age-matched sedentary controls.1 It was also observed that some particular sport disciplines improve the lung function better than others, these include swimming, and, as recently reported, basketball, water polo and rowing.2–4 Swimmers also achieve larger lung volumes and higher functional cardiorespiratory system capacity compared to other athletes.5,6 However, the impact of swimming (as a specific type of sport) on the development of the lung function has not yet been clearly established.
Aerobic exercise enables efficientt lung oxygen uptake, making the lungs work effectively by activating large muscle groups and raising the heart rate. In addition, swimmers perform strenuous underwater exercise holding their breath for prolonged periods.3 Respiratory muscles, including swimmer's diaphragm, are required to develop higher pressure, resulting from water immersion during the respiratory cycle, leading to functional strengthening of the muscles, as well as improvement in the chest wall elasticity, resulting in higher level of the lung function.3,6 However, the possibility that hereditary factors may have an influence on the larger lung volumes in swimmers cannot be ruled out. Recent studies have shown that swimmers present larger lungs, which could not be attributed to changes in height, fat free mass, maximal respiratory mouth pressures, alveolar distensibility, age at start of training, years of training, training time per week, distance per session, sternal length, or chest depth at total lung capacity.7
In the land-based sport activities, respiratory system is not usually considered to be a limitation factor for physical activity, but no extensive studies have been conducted to approve or rebut this statement in general.1,8
Spirometry is the crucial respiratory function assessment test, as a standardized and reproducible method for estimating the respiratory mechanism and pulmonary ventilation. Spirometric values determined in athletes usually refer to standards (i.e. standardized predicted values) for the average population of healthy subjects, as recommended by international organizations, such as the European Respiration Society (ERS), European Commonwealth of Coal and Steel (ECCS) or the American Thoracic Society (ATS).9,10,11
The first aim of this study was to compare lung volumes in elite athletes, e.g. swimmers (representing water-based sport activity) and football players (representing land-based sport activity) and their age- and sex-matched sedentary controls; the second aim was to examine whether the training factors have an influence on the pulmonary function in swimmers in controlling anthropometric features.
Materials and methodsParticipantsThree hundred and nine elite athletes (thirty eight swimmers) and one hundred age- and sex- matched sedentary controls were included in the study. An elite athlete was defined as a male athlete participating in international competitive tournaments, with at least a five year history of active playing and with at least 15h of training per week. Sedentary controls were medical students, conditioned to not being connected with any particular sport activity and with no regular exercise program.
Data concerning age at the beginning of training, training period (years) and weekly amount of personal training (hours) were recorded. Each athlete's personal training was assessed as the number of training sessions per week and hours per session, as obtained by questionnaire and interview and presented as total hours of weekly personal training.
The exclusion criterion was any kind of pulmonary disease. All tests were performed in laboratory settings with the same instruments and techniques.
MeasurementSpirometry was performed using the (Turninac, Pneumotah) Pony FX (Cosmed Pulmonary Function Equipment, Italy). Subjects underwent the test in a sitting position, wearing a nose clip. After a maximal inhalation, they sealed their lips around the mouthpiece and exhaled as hard and as fast as possible. They were encouraged to continue exhaling for at least six seconds so that forced expiratory volume for one second (FEV1) and FVC could be measured. Tests were repeated three to five times until the two highest recorded values-forced vital capacity (FVC) and FEV1-varied by less than 3%. Direct measurements included FVC (liters), FEV1 (liters), and peak expiratory flow-PEF (liters/second). The forced expiratory ratio (FEV1/FVC×100) was also calculated (%).10 All of the above measurements were carried out under standard environmental conditions, by continuously measuring the temperature, humidity and atmospheric pressure which enabled comfort temperature (between 18°C and 22°C), the atmospheric pressure of 760mmHg, and a relative atmospheric humidity of 30 to 60%.
Body mass (kg; Seca 761 scales, ±0.5kg; Seca Co., Germany) and body height (m; Cranlea JP60 portable stadiometer, +0.001m; Cranlea & Co) were measured using standardized anthropometric techniques. Body mass index (BMI) was calculated for all participants as the ratio of body mass (kilograms) divided by the body height (meters) squared. The body fat percentage (BF %) was measured using the bioimpedance segmental body composition analyzer (BC-418 Segmental Body Composition Analyzer, Tanita, IL, USA).
Ethical approvalThe research protocol was approved by Institutional Review Board for medical ethics and complied with the guidelines of the Declaration of Helsinki.
Statistical analysisPulmonary test results were presented by descriptive methods of statistics, as measured values (liters) and as values calculated in relation to the predicted values (percentages). Kolmogorov–Smirnov test was used to pre-test data distribution. Kruskal–Wallis one way ANOVA test was used to evaluate differences among groups; Mann–Whitney U test was used for the inter-group differences. Pearson correlation coefficient was used to determine correlation between anthropometric features and the measured pulmonary function indices. The analysis of covariance (ANCOVA) test was used to determine the effects of training (evaluated separately according to age at the beginning of training, training period and weekly amount of personal training) on the respiratory function indices in swimmers, when controlled for anthropometric features (height and weight). The level of significance was set at 95% (one star) and 99% (two stars) for all statistical analyses, using SPSS 20.0.
ResultsAge at the beginning of training was 9.4 (2.6) for swimmers and 8.4 (2.1) for football players, which significantly differed (p=0.035). Training period was 12.8 (3.0) years for swimmers and 11.9 (3.9) years for football players with no statistical difference. The amount of personal training was 22.0 (7.9) and 21.1 (5.2)h per week for swimmers and football players, respectively (with no significant difference).
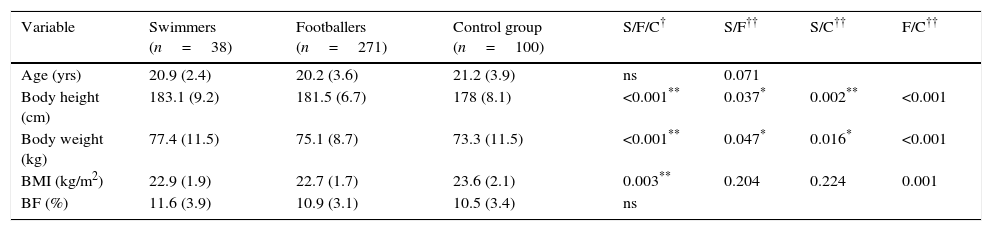
Patient characteristics are given in Table 1. Groups did not differ in relation to age and body fat. Both groups of athletes were significantly taller and weighed more than the control group. Among athletes, swimmers were taller and heavier than the football players. Athletes did not differ in BMI, but controls had higher BMI than the football players.
Demographic and anthropometric characteristics of both groups of athletes and the control group.
| Variable | Swimmers (n=38) | Footballers (n=271) | Control group (n=100) | S/F/C† | S/F†† | S/C†† | F/C†† |
|---|---|---|---|---|---|---|---|
| Age (yrs) | 20.9 (2.4) | 20.2 (3.6) | 21.2 (3.9) | ns | 0.071 | ||
| Body height (cm) | 183.1 (9.2) | 181.5 (6.7) | 178 (8.1) | <0.001** | 0.037* | 0.002** | <0.001 |
| Body weight (kg) | 77.4 (11.5) | 75.1 (8.7) | 73.3 (11.5) | <0.001** | 0.047* | 0.016* | <0.001 |
| BMI (kg/m2) | 22.9 (1.9) | 22.7 (1.7) | 23.6 (2.1) | 0.003** | 0.204 | 0.224 | 0.001 |
| BF (%) | 11.6 (3.9) | 10.9 (3.1) | 10.5 (3.4) | ns |
Values are expressed as mean (SD) unless otherwise specified S, swimmers; F, football players; C, controls; ns, non-significant; BMI, body mass index; BF, body fat.
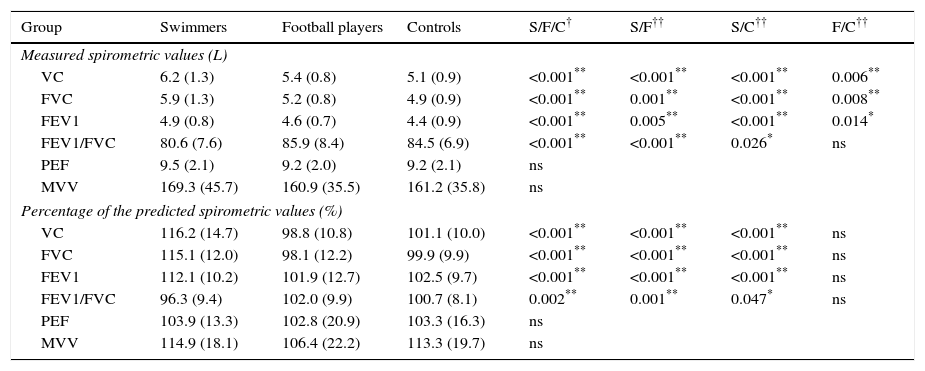
Mean values of the measured spirometric indices are shown in Table 2. Both groups of athletes had significantly higher values of the VC, FVC and FEV1 (measured in liters) than the control group. Swimmers had higher values for all of the mentioned indices in comparison to football players. The FEV1/FVC ratio was statistically higher in swimmers compared to both the football players and the control group. There was no difference in measured values of PEF and MVV in the examined groups.
Pulmonary function values for both groups of athletes and the control group.
| Group | Swimmers | Football players | Controls | S/F/C† | S/F†† | S/C†† | F/C†† |
|---|---|---|---|---|---|---|---|
| Measured spirometric values (L) | |||||||
| VC | 6.2 (1.3) | 5.4 (0.8) | 5.1 (0.9) | <0.001** | <0.001** | <0.001** | 0.006** |
| FVC | 5.9 (1.3) | 5.2 (0.8) | 4.9 (0.9) | <0.001** | 0.001** | <0.001** | 0.008** |
| FEV1 | 4.9 (0.8) | 4.6 (0.7) | 4.4 (0.9) | <0.001** | 0.005** | <0.001** | 0.014* |
| FEV1/FVC | 80.6 (7.6) | 85.9 (8.4) | 84.5 (6.9) | <0.001** | <0.001** | 0.026* | ns |
| PEF | 9.5 (2.1) | 9.2 (2.0) | 9.2 (2.1) | ns | |||
| MVV | 169.3 (45.7) | 160.9 (35.5) | 161.2 (35.8) | ns | |||
| Percentage of the predicted spirometric values (%) | |||||||
| VC | 116.2 (14.7) | 98.8 (10.8) | 101.1 (10.0) | <0.001** | <0.001** | <0.001** | ns |
| FVC | 115.1 (12.0) | 98.1 (12.2) | 99.9 (9.9) | <0.001** | <0.001** | <0.001** | ns |
| FEV1 | 112.1 (10.2) | 101.9 (12.7) | 102.5 (9.7) | <0.001** | <0.001** | <0.001** | ns |
| FEV1/FVC | 96.3 (9.4) | 102.0 (9.9) | 100.7 (8.1) | 0.002** | 0.001** | 0.047* | ns |
| PEF | 103.9 (13.3) | 102.8 (20.9) | 103.3 (16.3) | ns | |||
| MVV | 114.9 (18.1) | 106.4 (22.2) | 113.3 (19.7) | ns | |||
Values are expressed as mean (SD) unless otherwise specified; S, swimmers; F, football players; C, controls; ns, non-significant; VC, vital capacity; FVC, forced vital capacity; FEV1, forced expiratory volume in the first second; FEV1/FVC-Tiffeneau-Pinelli index; PEF, peak expiratoy flow; MVV, maximum voluntary ventilation.
Measuring the percentage of the predicted spirometric values, swimmers had statistically higher values of VC, FVC, FEV1 and FEV1/FVC, compared to both the football players and the controls, as the latter two showed no in-between differences in the above mentioned parameters.
There was significant positive correlation for each of the following anthropometric features: age, body weight and body height and each of the following pulmonary parameters: VC, FVC, FEV1 and PEF when evaluated separately for swimmers, football players and the control group. Age, body weight and body height also positively correlated with MVV in footballers and controls, but not in the group of swimmers. On the other hand, negative correlation was found between FEV1/FVC and age, body weight and body height for each of the three investigated groups.
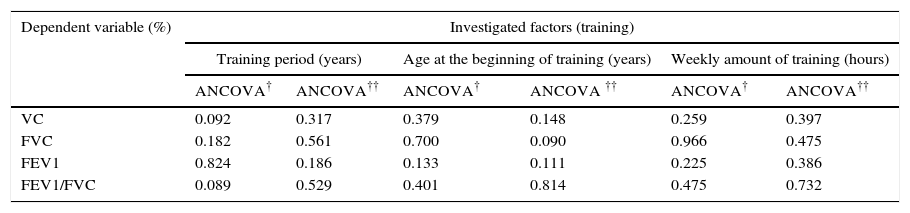
The influence of training factors on the pulmonary function indices in swimmers, when controlled for the anthropometric features, is shown in Table 3. Levene's test was used to pretest homogeneity of the variance and showed that the error variance of the dependent variable was equal across groups. The ANCOVA interaction test was run afterwards, showing that there was no training effect by anthropometric features on pulmonar capacity. Finally, the ANCOVA main test was used to evaluate the influence of training on the pulmonary function indices when controlled for the anthropometric features and showed that there was no influence of any of the following training factors: period of time, age at the beginning of training and weekly amount of personal training on the percentage of the predicted spirometric values: VC, FVC, FEV1 and FEV1/FVC in swimmers.
Analysis of covariance (ANCOVA) test, evaluating the influence of training on the pulmonary function indices in swimmers, when controlled for the anthropometric features.
| Dependent variable (%) | Investigated factors (training) | |||||
|---|---|---|---|---|---|---|
| Training period (years) | Age at the beginning of training (years) | Weekly amount of training (hours) | ||||
| ANCOVA† | ANCOVA†† | ANCOVA† | ANCOVA †† | ANCOVA† | ANCOVA†† | |
| VC | 0.092 | 0.317 | 0.379 | 0.148 | 0.259 | 0.397 |
| FVC | 0.182 | 0.561 | 0.700 | 0.090 | 0.966 | 0.475 |
| FEV1 | 0.824 | 0.186 | 0.133 | 0.111 | 0.225 | 0.386 |
| FEV1/FVC | 0.089 | 0.529 | 0.401 | 0.814 | 0.475 | 0.732 |
All values are expressed as p values.
Higher volumes of VC, FVC and FEV1 were found in swimmers compared to both the football players and the control group (measured in liters and in percentages). The results of the present study support the previously published work which showed increased lung volumes in swimmers compared to land based sport disciplines and sedentary controls.5,12,13 In our study, higher lung volumes were found in football players compared to their sedentary counterparts when measured in liters, but no difference was observed in percentages. The present study supports the idea that physical training has a positive impact on the lung ventilatory function, as reported by other studies.2,14,15 The next question is whether larger lung volumes and capacities in athletes are due to their previously determined anthropometric features (height and weight), or due to training.5,7
It was previously reported that swimmers tend to be taller and to have higher bi-acromial breadths than their peers with the same body weight.5 Indeed, the swimmers in our study were taller and heavier than both football players and controls, and had greater lung volumes, accordingly. Anthropometric features could have provided advantages in numerous training techniques, leading to strengthening of the respiratory muscles and improving the lung function in swimmers, in addition to swimming itself.16,17 So, the question arises as to whether larger lung volumes in swimmers are due to their genetics or are developed by training.18,19 Prior studies reported that swimmer's anthropometric characteristics are mostly influenced by their genetic inheritance.5 This is likely to be true, bearing in mind the possibility that swimmers perform better and succeed in this specific type of sport simply because they are positively selected, because they were born with appropriate characteristics.
Our study adds to positive correlation between anthropometric features and respiratory function parameters, as was shown in each of our three investigated groups. Excluding the influence of anthropometric indices, we have found that training factors (training period, age at the beginning of training and weekly amount of personal training) did not influence the lung volumes in swimmers. Furthermore, despite the fact that football players started with intensive training earlier than swimmers (at age of 8.4 vs 9.4), percentages of their lung volumes were lower than that of swimmers and did not differ from the control group.
Besides age, sex, race, height and weight, pulmonary function depends on numerous factors in physically normal individuals: the balance between lung recoil and chest elasticity, (determining the mid-position at the end of spontaneous expiration and the coordinated neuro-muscular function to maintenance the effort); strength of the thoracic and abdominal muscles, individual posture and lung elasticity. Unlike other sports, swimming activates the whole body system muscles, with excessive usage of the chest wall and abdominal muscles, characterized by periods of prolonged holding the breath causing intermittent hypoxia, as a result of the specific way of training. Swimming also differs from other sport disciplines in numerous ways; it is performed in the horizontal position compared to the other sports’ vertical posture, external pressure is higher because the density of the surrounding medium is higher than that of air; and also the water heat conduction is higher than that of air.20–23
ConclusionElite swimmers had larger lung volumes and were taller and heavier when compared to football players and the control group. Lung volumes in land-based activities (football players) and sedentary controls did not differ. Influence of age, height and weight on the lung function was positive for both groups of athletes and the control, sedentary group. According to the present study, when controlled for the anthropometric features, lung volumes in swimmers cannot be explained by training period, age at the beginning of training or weekly amount of personal training. Therefore, larger lung volumes in swimmers could be attributed to their genetic predisposition, or to a special way of training, which is a specific way of breathing, specific training position or the specific surrounding medium.
Study limitationsStudy involved only males subjects. In Serbia, there are only 38 elite swimmers who compete at an international level.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Conflicts of interestThe authors have no conflicts of interest to declare.


