




Patients present poor knowledge and skills about their respiratory disease and inhaler device. We aimed to: (1) evaluate COPD and asthmatic patients... ability to manage inhaled drugs (2) identify differences among devices and (3) correlate clinical data with patient ability.
Material and methodsPatients (n=134) admitted for pulmonary rehabilitation (PR) were given an ad-hoc questionnaire covering 0% as the worst and 100% the best value of global ability (indicating the sum of knowledge and skills in managing inhaled drugs) at baseline (T0) and discharge (T1). Educational program was provided during PR. Setting of rehabilitation, age, sex, diagnosis, spirometry, CIRS score, level of autonomy to use medications, if na..ve about PR, educational level, and number/type of prescribed inhaled drugs were recorded.
ResultsMost patients used 1 drug while 37% used 2 drugs. DPIs were the main device prescribed. At baseline, patients... mean level of knowledge and skills were 73% and 58%, respectively. There was a significant difference in level of skills (p=0.046) among device families, DPIs resulting worst and pMDIs best. Global ability, skills and knowledge improved after educational support (p<0.001) but did not reach the optimal level, 88%, 87% and 89%, respectively. Baseline global ability was positively correlated to female gender, younger age, previous PR access, outpatient status, higher education level and GOLD D class.
ConclusionsAt hospital admission, global ability was not optimal. Education may improve this, irrespective of the type of device used, in particular in male, elderly, na..ve to PR, low educational level patients.
Asthma and chronic obstructive pulmonary disease (COPD) are chronic inflammatory pulmonary diseases affecting millions of people worldwide.1 Inhaled therapy can be delivered via nebulizers, pressurized metered-dose inhalers (MDIs), dry powder inhalers (DPIs), and soft mist inhalers (SMIs). Studies consistently report that many patients with asthma and COPD do not use their inhaler devices correctly.2,3 Indeed, medications cannot be effective if they do not reach the sites they are intended to target.4,5 Poor inhaler technique stems from the fact that patients often poorly understand the purpose of and how to use their inhalation device.6 Poor adherence is common, with 50% or more of patients with asthma and COPD not taking their inhaled therapy as prescribed or instructed.7,8 Non adherence can further perpetuate poor technique and can lead to costly exacerbations and worsening disease.7,8 A comprehensive patient education, including device training, can improve outcomes.9,10 However, even with training, not all patients are able to use their inhalers correctly.11
The aims of this study were: (1) to evaluate with a simple interview the global ability, knowledge and skills in managing inhaled drugs before and after an educational program during rehabilitation for obstructive respiratory disease patients; (2) to compare, if any, differences among the prescribed devices; and (3) to correlate clinical and anthropometric data with the overall ability to manage drugs.
MethodsThis observational qualitative study considered a cohort of patients attending the Respiratory Unit of the Istituti Clinici Scientifici (ICS) Maugeri of Lumezzane (Bs), Italy. The study was conducted in a single center and approved by ICS Maugeri IRCCS Ethics Committe (EC 2322; 16 July 2019). All participants were informed and gave their written consent to participation.
PatientsConsecutive patients aged >18 years with a diagnosis of COPD or severe asthma were eligible for enrolment. COPD and asthma were defined according to Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria12 and Global Initiative for Asthma (GINA) guidelines.13 Patients were admitted either to an inpatient program with an average stay of 25 (SD 3) days or an outpatient program attending no less than 22 rehabilitative sessions with 2 or 3 weekly accesses over a 2-month period. Indication and prescription for pulmonary rehabilitation (PR) was not based only on FEV1 value, but according to a previously published internal triage,14,15 generating a Pulmonary Rehabilitation Decisional score (PRDS). PRDS considers several items such as lung function, clinical parameters, disability, frailty, and participation in ADLs and has been used for staging the clinical priority of PR prescription and choosing the PR setting (inpatient or outpatient). Anyway, all patients coming from acute hospitals have been inserted in the ..úinpatient group..Ñ. Patients were followed by a pulmonologist and nurse case managers, nurses, respiratory therapists and others pulmonologists. The proposed PR programs were based on classical guidelines indications16 based on aerobic training, calisthenics, lower and/or upper limb selective muscle strengthening, balance training, inspiratory muscle training and secretion assistance when indicated. During the PR program drugs adjustments (in terms of quality and quantity) were carried out according to guidelines and clinical needs.
Exclusion criteria were: dyspnea at rest with need for acute hospitalization, oncological disease, terminal illness, neuromuscular degenerative diseases, severe orthopedic diseases, subject bedridden or confined to a wheelchair, and altered cognitive status measured by MMSE17<22.
InterventionDevelopment of the interviewTo obtain a questionnaire with face validity based on expert opinion involving a structured process of consensus, we engaged key stakeholders (4 doctors and 4 nurses) from among health staff employed in the rehabilitation field of our Institute. We performed a systematic review of the COPD literature identifying items to use for the questionnaire and prepared a preliminary draft of questions. During the meeting, using a Delphi-like procedure, we asked the experts to rate the accordance of preselected items on a 5-point Likert scale (0=totally disagree; 1=disagree; 2=sufficiently agree; 3=moderately agree; 4=totally agree). Consensus was considered when more than 75% of the respondents rated each item as totally agree. Finally, the focus group checked that the wording of each question was simple, clear, and comprehensible (details in supplementary material).
The final tool consisted of 8 questions enquiring about: the name of the drug/drugs, dosage prescribed, time of administration during the day, ability to distinguish the drug/s from others, the usefulness, and how to prepare, use and replace the drugs (Fig. 1). The operator scored each item dichotomously, according to the patient's response, as knows/does not know or correct maneuver/incorrect maneuver (Fig. 1). The score for part A (representing the percentage of correct answers for knowledge) and that for part B (representing the percentage of correct maneuvers for skills) were added up to give a final total global ability score (A+B), 0% was the worst and 100% the best value of global ability (details in supplementary material).
Interview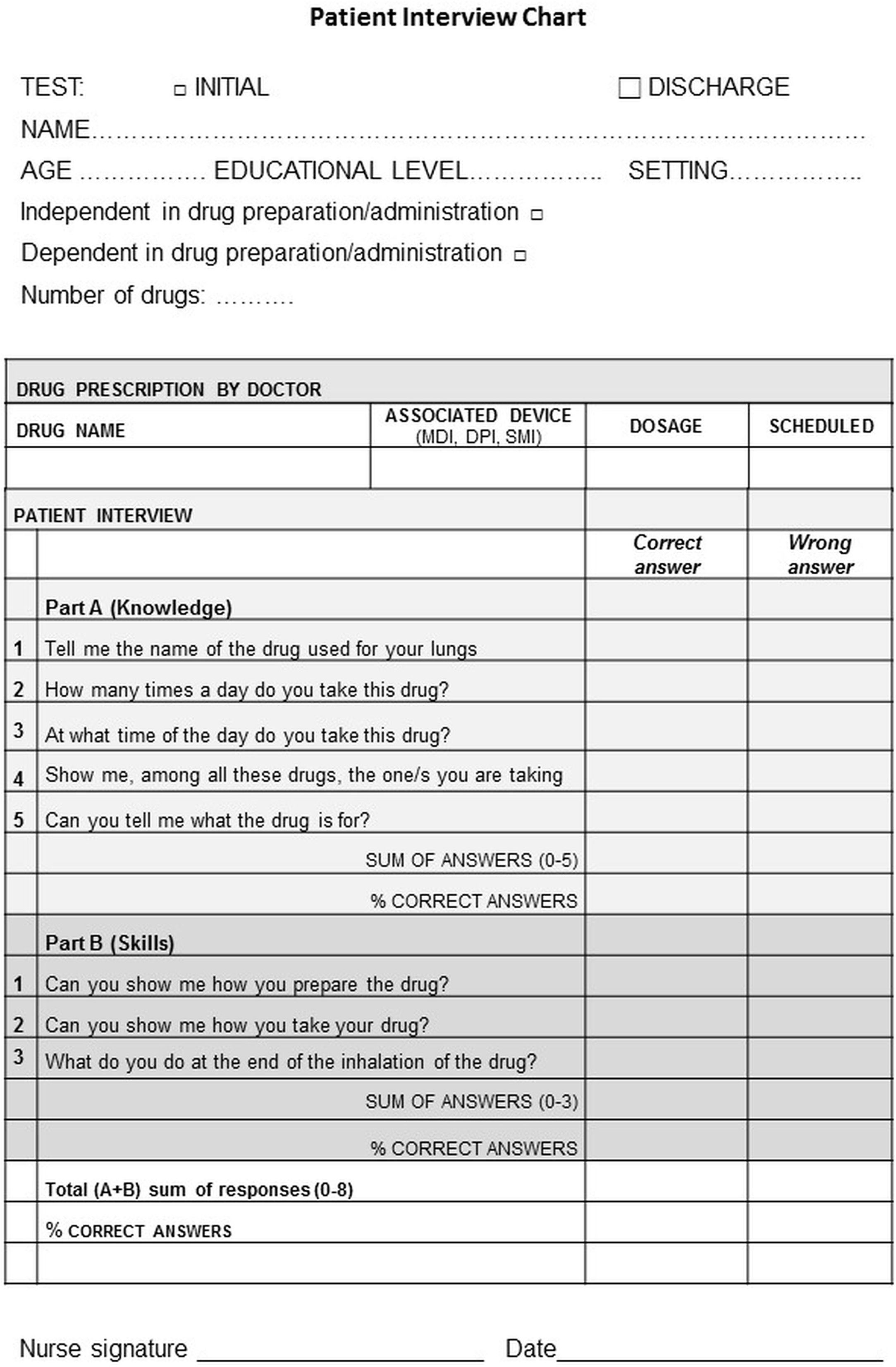
Before conducting the interviews, all nurse staff participated in a briefing session on how to conduct the interview in a standardized way. According to the previous literature18 a list of possible mistakes/error for incorrect drug use was prepared. Nursing staff used the list during his/her interview (details in supplementary material).
The score was calculated (T0) during a face to face visit and assigned to a nurse case-manager not involved in the educational program. Patients admitted for a PR program, either as inpatients or outpatients, underwent the interview at the time of admission or at their first/second access.
Education programAfter assigning the score and starting from the baseline level of knowledge and skills, 2 structured tailored educational meetings of 20min each (including reminders, motivation, reinforcement, demonstration, sheets and videos material) were given by a dedicated team of 4 nurses (2 for outpatients and 2 for inpatients), different from the case manager, to reinforce the knowledge and the correct use of the inhalation therapy, in such a way as to be able to intervene promptly and effectively if the therapy was not performed correctly (details in supplementary material).
The form for verification of change in knowledge and skills to inhalation therapy was re-administered to the patient on discharge (T1) by the same case-manager.
MeasurementsThe following data were collected: setting of rehabilitation, demographic data such as age, sex, definitive diagnosis of COPD based on spirometry, presence of comorbidities with the Cumulative Illness Rating Scale (CIRS),19 present/past data on FEV1 (% pred.) and forced vital capacity [FVC (% pred.)], if na..ve to PR, educational level (no education or elementary school vs. higher than elementary school), number and type of inhaled drugs routinely used, if the patient was generally autonomous in the use of drugs. Patients were defined as autonomous if they had an acceptable level of cognitive status and absence of dysphagia.
Statistical analysisStatistical analysis was performed using STATA 11 (StataCorp LLC, Texas 77845-4512 USA). Continuous variables were expressed as mean..standard deviation (SD). Binary and categorical outcomes were described as frequency and percentage in each group. A two-sample t-test comparing differences at baseline between groups and changes after education training was performed. To identify correlations between baseline characteristics and the risk of presenting a low baseline global ability (defining by value below the median of global baseline data), we performed a post hoc analysis to estimate the Odds Ratio (OR). A p value <0.05 was considered as statistically significant.
ResultsOne hundred and thirty-four patients were consecutively enrolled in the study. The time spent on the patient interview was 3.06..1.70min (range 1.51...6.55).
Table 1 shows baseline data of the patients. The majority of patients routinely used only one inhaled drug while 37% used 2 drugs (the majority of these had COPD). Almost all patients were autonomous regarding general use of their medication. No differences were found in device categories between COPD and asthma. The majority of patients used a DPI: Diskus (9%), Ellipta (19.8%), Genuair (23%), Nexthaler (5.7%), Turbuhaler (5.1%), HandiHaler (7.4%), Breezhaler (30.6%). Younger patients used MDIs more frequently while patients with lower FEV1% pred. more frequently used MDIs and SMIs. When compared to the whole group, SMI group (9.7%) included patients admitted in the 60% of the cases as inpatients, older (72..9 years), in 38% of cases with CRF and with higher cultural level (70% of cases). At discharge after PR, drug prescription was changed in 30% of COPD and 51% asthmatic patients, respectively (in all cases number and dosage of drugs were increased).
Baseline characteristics of patients.
| ALL | COPD | Asthma | p | |
|---|---|---|---|---|
| Patients, n | 134 | 107 | 27 | |
| Inpatient/outpatient, n | 49/85 | 42/65 | 7/20 | 0.199 |
| Age, years | 70.34 (8.26) | 70.18 (8.53) | 71 (7.20) | 0.646 |
| Gender (M/F), n | 92/42 | 75/32 | 17/10 | 0.475 |
| FEV1% pred. | 61.47 (25.27) | 55.12 (23.01) | 86.63 (16.90) | <0.001 |
| FVC % pred. | 84.51 (23.14) | 82.05 (23.14) | 94.30 (20.74) | 0.013 |
| FEV1/FVC | 59.22 (19.52) | 52.63 (14.74) | 85.37 (13.19) | <0.001 |
| GOLD A, % | 9.3 | |||
| GOLD B, % | 38.3 | |||
| GOLD C, % | 8.4 | |||
| GOLD D, % | 43.9 | |||
| GINA I, % | 7.4 | |||
| GINA II, % | 14.8 | |||
| GINA III, % | 48.1 | |||
| GINA IV, % | 22.2 | |||
| GINA V, % | 7.5 | |||
| Educational level (elementary), n (%) | 71 (53) | 52 (49) | 19 (70) | 0.103 |
| CIRS1, score | 1.70 (0.36) | 1.70 (0.37) | 1.69 (0.36) | 0.897 |
| MMSE, score | 25.29 (1.24) | 25.02 (1.37) | 26.33 (1.01) | 0.631 |
| Naive to pulmonary rehabilitation, n (%) | 48 (36) | 35 (33) | 13 (48) | 0.135 |
| Respiratory drugs routinaly used | 1.40 (0.52) | 1.48 (0.54) | 1.11 (0.32) | 0.001 |
| One, n (%) | 82 (61) | 58 (54) | 24 (89) | 0.004 |
| Two, n (%) | 50 (37) | 47 (44) | 3 (11) | 0.004 |
| Three, n (%) | 2 (2) | 2 (2) | 0 (0) | 0.004 |
| Autonomy in drug use, n (%) | 128 (96) | 105 (98) | 23 (85) | 0.004 |
| MDI, % | 20.15 | 19.63 | 22.22 | 0.764 |
| DPI, % | 70.15 | 72.90 | 59.26 | 0.166 |
| SMI, % | 9.70 | 18.52 | 7.48 | 0.083 |
FEV1=forced expiratory volume at first second; FVC=forced volume capacity; GOLD=Global Initiative for Chronic Obstructive Lung Disease; GINA=Global Initiative for Asthma; CIRS=Cumulative Illness Rating Scale; MMSE=mini-mental state examination; MDI=metered dose inhaler; DPI=dry powder; SMI=soft mist inhaler. Where undefined, number in parentheses refers to (SD).
Patients with low education level more frequently used MDIs. No differences in the devices used at admission were found concerning comorbidities and previous PR access.
All patients attended 2 educational sessions, 37.3% of COPD patients and 18.5% of asthmatic patients needed 3 educational sessions, because the dedicated nurses found these patients were still insecure and not yet ready to perform the final interview. Patients needing more than 2 sessions were older, with lower educational level, with lower MMSE and more na..ve to PR.
On hospital admission, knowledge, skills and global ability regarding inhaled drugs were not optimal with 69%, 74% and 83% of patients with level <100%, respectively. Mean and median global ability in percentage at baseline were 67.27..26.26 and 68.75 (IQR 50.0...87.5), and at discharge 88.06..18.82 and 100 (IQR 83.3...100) (p<0.001), with mean delta improvement 20.79..18.50. Fig. 2 (panel a) shows baseline (T0) and delta improvement at discharge (T1) in percentage of the global ability score and according to the components of skills and knowledge. The pre-to-post changes were all statistically significant (p<0.001) (panel a), the mean improvement in skills was 29.19..29.61 and in knowledge 15.60..20.17. In detail, 100 patients (75%) improved global ability, while 34 (25%) worsened or remained unchanged. As to skills ability, at discharge, 30% of patients were still unable to use their devices correctly.
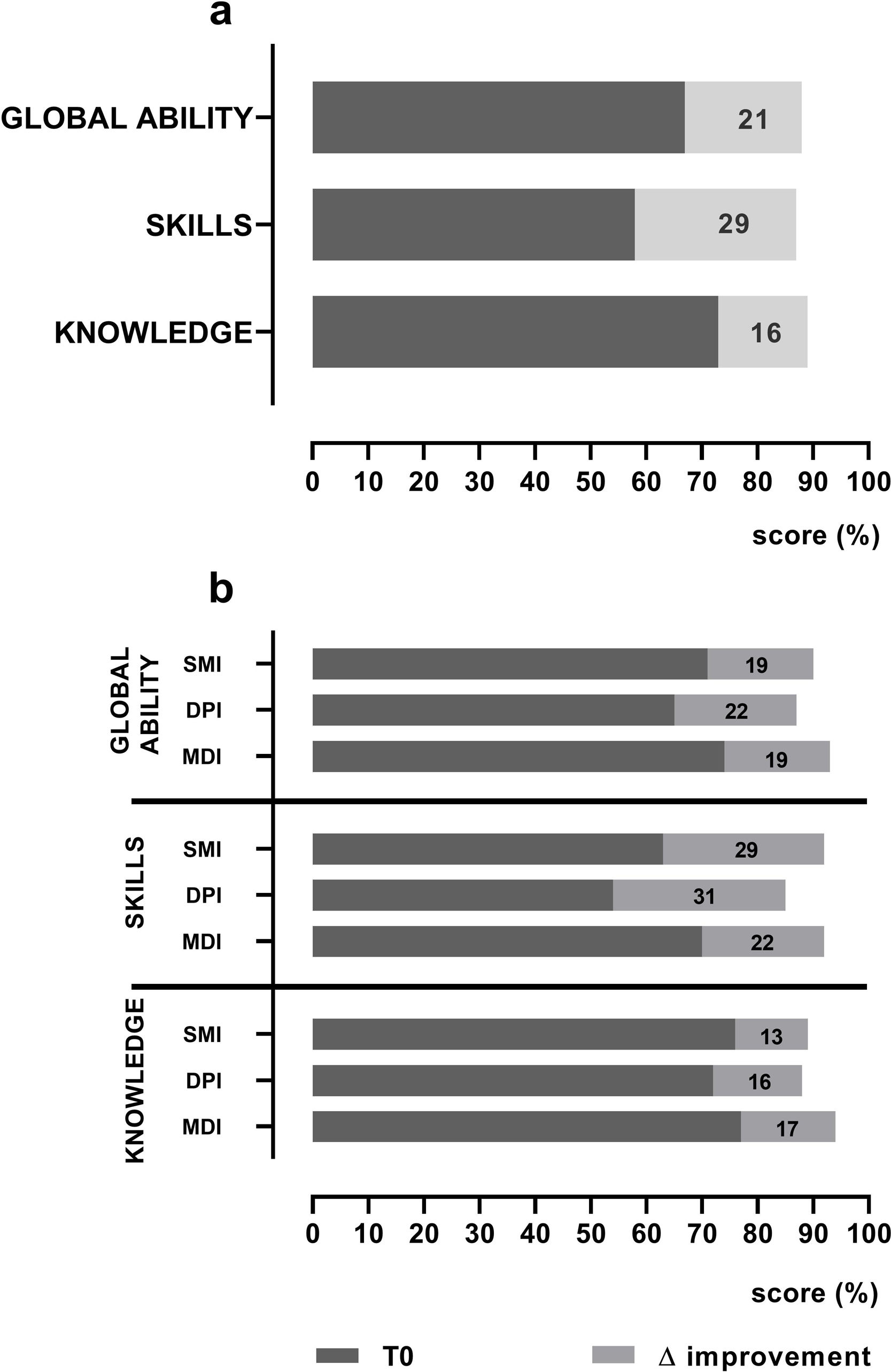
(panel a) shows baseline mean T0 score (dark bars) and mean delta score improvement at discharge (gray bars) in patient's global ability and the components of skills and knowledge. The pre-to-post changes (delta score improvement) were all statistically significant (p=<0.001); (panel b) shows baseline mean T0 scores (dark bars) and mean delta score improvement at discharge (gray bars) in global ability, in skills and knowledge according to different families of devices used. MDI=metered dose inhaler; DPI=dry powder inhaler; SMI=soft mist inhaler.
Fig. 2 (panel b) shows baseline values and delta improvement at discharge in global ability, skills and knowledge according to the 3 different families of devices tested (SMI, DPI and MDI). Differences in the patients... global ability at baseline were not significant among the devices tested (p=0.144). At baseline only, there was a significant difference (p=0.046) in the patients... level of skills in using different families of devices: the DPI family being the worst and the MDI the best; the delta skills improvement after education was otherwise not different (p=0.262). Patients... knowledge of devices at baseline and delta knowledge improvement after education were not significantly different (p=0.516 and p=0.745, respectively). At discharge global ability, skills and knowledge did not reach the optimal level being 88%, 87% and 89% respectively.
Table 2 shows the Odds Ratios risk to predict a low baseline global ability to use inhaler devices (less than the median value of 68.75). While female gender, younger age, previous PR access, outpatient status, higher education level and being into GOLD D class showed a protective effect on low baseline global ability to use inhaler devices, diagnosis, prior clinical classification of autonomy, FEV1%<30, CIRS>1.6, type of device, and use of more than one inhaled drug did not influence baseline global ability.
Odds ratio (OR) to predict a low baseline global ability (less than the median value of 68.75).
| OR | Standard error | p | 95% CI | |
|---|---|---|---|---|
| Male | 2.38 | 0.92 | 0.034 | 1.111...5.098 |
| Age>65 years | 2.35 | 0.954 | 0.037 | 1.064...5.212 |
| Not na..ve to PR | 0.11 | 0.04 | <0.001 | 0.049...0.262 |
| Outpatient | 0.14 | 0.06 | <0.001 | 0.064...0.335 |
| Higher educational level | 0.24 | 0.89 | 0.026 | 0.118...0.501 |
| GOLD D class | 0.33 | 0.13 | 0.004 | 0.156...0.708 |
PR=pulmonary rehabilitation, CI=confidence interval.
This study has demonstrated that at hospital admission knowledge and skills regarding inhaled drugs were not optimal (69% and 74% of patients with level <100%, respectively). A simple, clear and short interview at admission and discharge may be a good tool to monitor patients... knowledge and skills. A tailored educational program may strongly improve this gap, irrespective of the type of device used. Based on our findings, drugs education should be targeted particularly at patients who are male, elderly, na..ve to PR, with a low educational level.
Obstructive respiratory disease patients are poorly adherent to inhaler therapy. Low adherence was associated with age, current smoking status, number of respiratory drugs prescribed and poorer quality of life,20 patients... perception of their health and medication effectiveness, and the presence of depressed mood and comorbidities.21
Eighty-two percent of COPD patients claimed to understand their disease and treatment, needed continuous education regarding inhalation devices.22 The Chronic Obstructive Pulmonary Disease knowledge Questionnaire (COPD-Q)23 explores risk of infections, use of oxygen, utility of drugs, prevention, correct time to use long-acting drugs, symptoms, smoking cessation, SABA use, and disease time course. In our study, we proposed a short simple interview oriented exclusively on drugs knowledge and skills. The rationale of the questionnaire is to focus deeply on whether patients are able to remember the name, dosage, time of use, utility and can recognize their device amongst several other devices and perform correctly the preparation, use and post-use recommendations.
In outpatient settings mistakes using inhaler devices has been found in a range of 6...71%, with 40% of patients presenting at least one vital mistake.24...28 Muller et al.29 found that 51.8% of patients present at least one mistake about using their devices. Molimard et al.,8 in a large cohort of patients outside of hospital, assessed inhaler device handling and its association with exacerbations. Handling errors were found in over 50% and exacerbations were less frequent in the absence of errors, while they doubled in the presence of critical error. Melani et al.30 in a large cohort of both asthmatic and COPD patients found that critical mistakes were no fewer in DPIs than in MDIs: in 12% for MDIs vs. 35% for Diskus and HandiHaler, and 44% for Turuhaler. In patients referred for a chest visit, inhaler-specific errors were as follows: Aerolizer 9.1%, Diskus 26.7%, HandiHaler 53.1% and Turbuhaler 34.9%.31
Only one study was conducted in an inpatient setting...it found that misuse was common in COPD (86% with MDI and 71% with Diskus).32 The lower level of misuse and errors found in our sample (60% for drugs skills) may be due to the particular rehabilitative setting, i.e. 64% of patients were not na..ve to PR, probably already confident with regard to drug education, with mixed diseases (asthma and COPD) and attending PR as both out- and inpatients. DPIs derive the energy for the emptying of the drug system from the user inspiratory flow: the failure to achieve a forceful inspiratory flow through a device was the most common critical mishandling error with DPIs in Melani et al....s study.30 In fact, in our study, COPD patients with a DPI were less able than patients with an MDI or SMI to use their devices, probably due to their severe functional limitation.
Critical errors and inability to improve after an education program found the following factors: older age,30,31,33 lower schooling30,33 and lack of instruction received,30,31,33...35 cognitive impairment or dyspraxia,36 use of 2 or more inhalers,34,36 and severity of airway obstruction.31 Our study confirms that age, lack of a previous educational program, and low level of education are negative predictors for drugs use ability; as a novel finding, we also demonstrated that female gender and outpatient regime (as opposed to inpatient) are protective factors. It is noteworthy that female patients seem to do better: possible explanations are that this group presented a higher cultural level (in 57% of cases) and fewer na..ve to PR (14%) when compared to males (43% and 40%, respectively). At the same time, it is not unexpected that outpatients group was better than inpatients due to a lower age (70..8 years old), a better level of airway obstruction (67..24% pred), more frequently with asthma (23%) and with a very low number of patients unable to use drugs (2.3%). Finally, it is interesting that only the more severe patients belonging GOLD D class presented a lower risk of having global inability: the possible explanation is that this group had attended previous PR program and education in the 76% of cases and, being more symptomatic, used more drugs with a higher adherence.
The lack of education by health caregivers on inhaler technique significantly increases the risk of misuse for all the studied devices.30,37 One study assessed errors with different devices in asthmatic and COPD patients after they had read the patient information leaflet:24 fewer COPD patients made critical errors with Ellipta (5%) than with other devices, and most patients (57...70%) did not require health-operator instructions using Ellipta, but instructions were required for Diskus (65%), MDI (85%), Turbuhaler (71%), HandiHaler (62%) and Breezhaler (56%).
Different training programs of diverse intensity and content (individual interviews about beliefs and behavior related to adherence, information about the illness and training about inhalation techniques, video) have been proposed, with patient skills... improvement ranging from 20 to 79%.26,35,38...40 In our sample, the mean improvement in skills was 29.19% while that in knowledge was 15.60%: these delta differences are clearly related to lower baseline values allowing more space for improvement (Fig. 2).
Limitations and strengthsLimitations of the study are the small sample size, the subjective basis of our findings (based on researcher-s judgment), the lack of a comparison control group and the fact that knowledge and skills measurement were not related to clinical outcomes. Another limitation is the use of a questionnaire with a dichotomous yes/no answer where the different skill capacity steps depended on a single answer grouped together. Strengths of our study are: (1) the simplicity of a questionnaire exclusively dedicated to drugs knowledge and skills; (2) the relatively short time needed to administer it, favoring its potential for routine use; (3) the comparison among different devices available in the market and (4) the presented data on a selected population admitted to a rehabilitative center.
ConclusionsThe findings were predominantly confirmatory of previous literature covering patients... lack of skills and knowledge about inhaled drugs, anthropometric, clinical and functional features which influence patients... global ability. The study adds that an educational program may improve this gap, irrespective of the type of device used, in patients who are male, elderly, na..ve to PR, with a low educational level.
Author contributionsMV, MF, EM, LC designed the study and draft the manuscript.
MF, EM, LC performed educational assessment and reviewed the manuscript.
MP and LB performed statistical analysis and reviewed the manuscript.
GB, CZ, AP, DF performed clinical assessment and reviewed the manuscript.
All the Authors approved the definitive version of the manuscript and declare that questions related to the accuracy or integrity of any part of it have been appropriately investigated and resolved.
Conflict of interestMV declares conflict for consultancy for or receipt of speaker's fees from Boeheringer; all the other Authors have no conflict of interest to disclose.
This work was supported by the Ricerca Corrente funding scheme of the Ministry of Health, Italy. The authors thank Rosemary Allpress for English revision, Laura Comini and Adriana Olivares for editing and technical assistance.
The following are the supplementary data to this article:



