



Dear Editor,
Benign tracheobronchial tumors account for only 1.9% of pulmonary tumors and a very small number of tracheobronchial fibroepithelial polyps have been reported in the literature so far.
The authors report the case of a 45-year-old man, active smoker, admitted with fever, purulent sputum and pleuritic chest pain for four days. He also referred progressive dyspnea on exertion, orthopnea and cough with mucoid sputum for the last 3 months. Physical examination revealed an oxygen saturation of 92% on room air and decreased breathing sounds on the lower half of the right hemithorax on chest auscultation.
Chest X-ray showed a heterogeneous opacity in the right lower lobe with an ipsilateral mediastinum deviation. The patient was started on antibiotics as community acquired pneumonia was initially assumed. Because there was neither clinical nor radiological improvement after 5 days of treatment, a chest computed tomography scan was performed showing obliteration of right main bronchus and consolidation of right inferior and middle lobes. Flexible bronchoscopy revealed a 2 cm pedunculated, glossy and lobulated lesion with implantation base on the right upper lobe carina, totally obstructing the right main bronchus and protruding to the trachea (Figure 1). As rigid bronchoscopy was readily available it was then performed and the lesion was fully removed at once with a biopsy forceps. Nd-YAG LASER was applied to the base of the lesion. The patient was discharged after 2 days, asymptomatic and with a normal chest X-ray. Histological examination revealed a respiratory epithelium with focal Malpighi metaplasia, with an axis containing many congested and dilated vessels, surrounded by stroma with variable collagenization, and lymphoplasmocytic inflammatory infiltrate accompanied by several mast cells, which established the diagnosis of a fibroepithelial polyp (Figure 2).
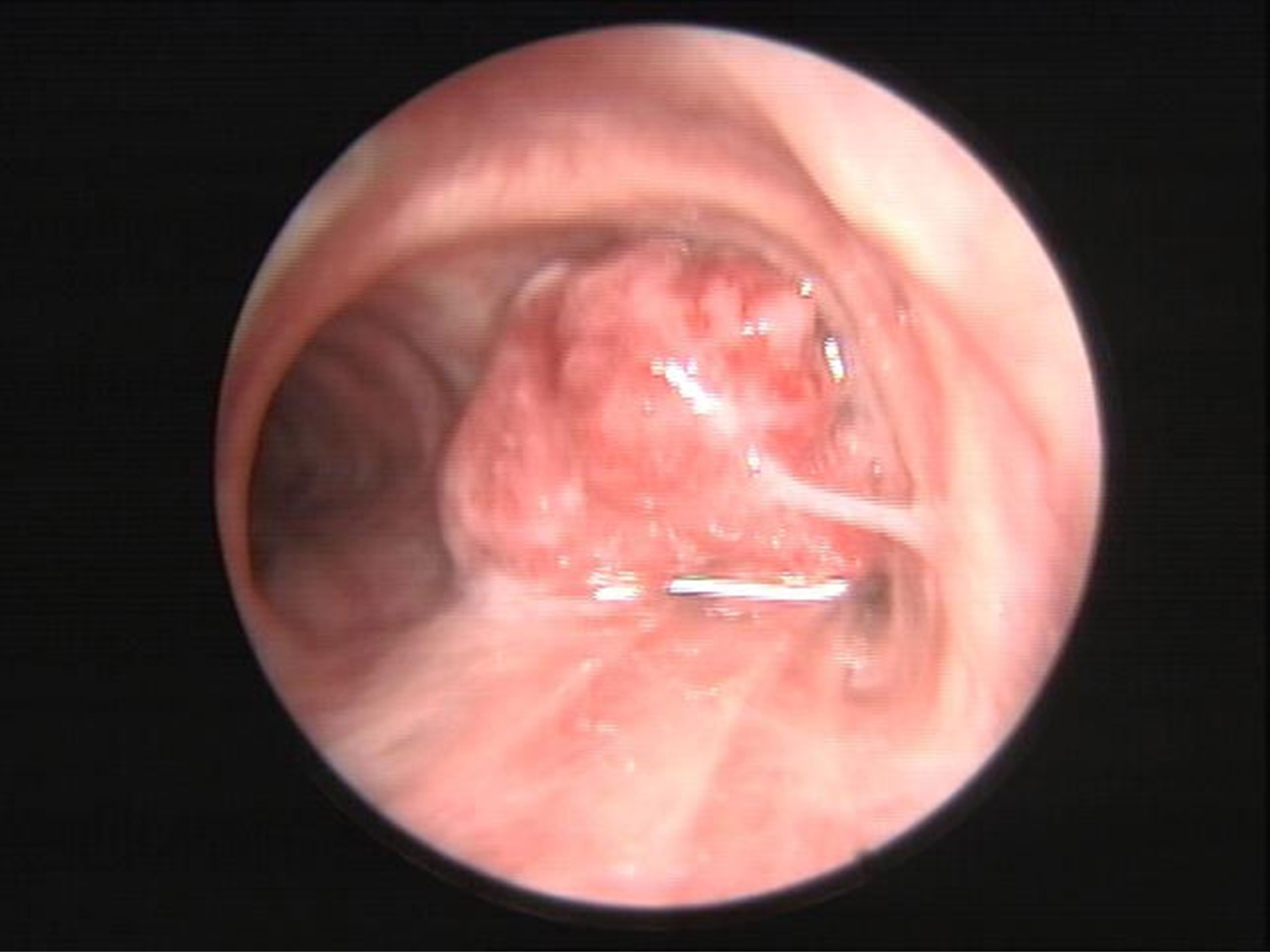
Figure 1. A 2 cm pedunculated, glossy and lobulated bronchial fibroepithelial polyp obliterating the right main bronchus.
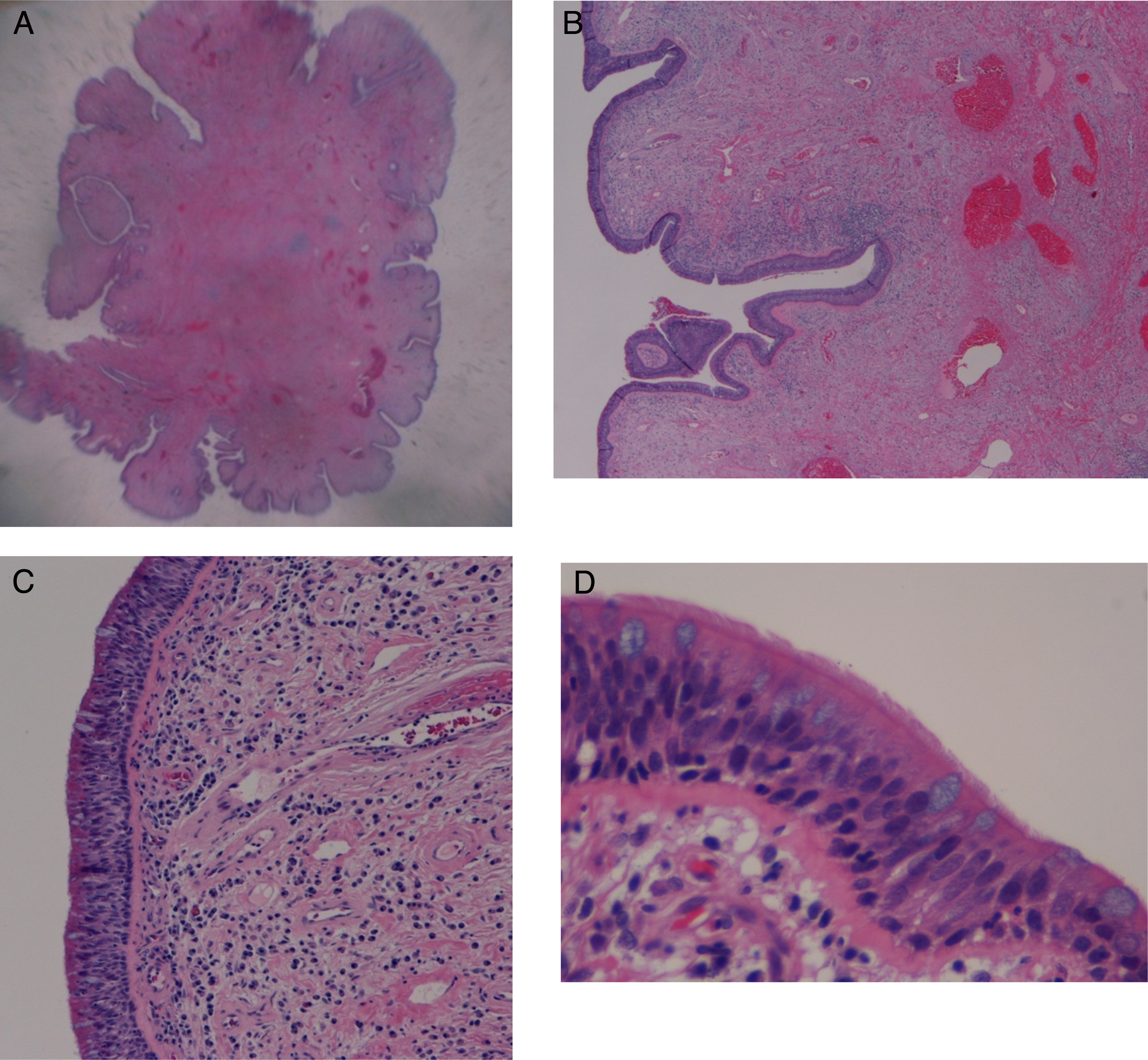
Figure 2. (A and B) Low power view, hematoxylin and eosin staining showing a polypoid lesion with a fibrovascular connective tissue axis; (C and D) high-power view, hematoxylin and eosin staining, showing a ciliated cylindrical epithelium with an inflammatory infiltrate.
A recent review on endotracheobronchial fibroepithelial polyps has found only 24 cases in the literature.1 It is a common type of tumor in the skin and genitourinary tract but very rare in the tracheobronchial tree.2, 3
Fibroepithelial polyps consist of fibrovascular stroma covered by normal respiratory or squamous epithelium with or without few inflammatory cells and adipocytic components.4 They are histologically different from papillomas which are frequently related to human papilloma virus and have neoplastic potential.3 Macroscopically, many of them are lobulated in contour, sometimes resembling a blackberry.4
The etiology of this entity remains unclear but it is thought that chronic inflammatory processes may be the principal causal factors. In the literature, there are reports of cases of endobronchial fibroepithelial polyps associated with chronic smoke inhalation, asthma, thermal injury, bronchiectasis, foreign body aspiration and titanium tetrachloride injury.3 Recurrence was reported in only one case.1
The symptoms will depend on the size and location of the polyp. Intratracheal tumors may be asymptomatic especially if small, but they may manifest with pseudoasthmatic wheezing, cough, dyspnea, or hemoptysis. Endobronchial tumors are frequently symptomatic, often causing partial or complete bronchial obstruction, which may result in recurrent pneumonias, bronchiectasis, unilateral wheezing, atelectasis, postobstructive pneumonitis, postobstructive hyperinflation, and occasionally hemoptysis.5
Treatment varies according to the size, hardness, presence of adjacent vessels and location. Some authors advocate that small lesions which are only responsible for a few symptoms can be treated with corticosteroids and antibiotics.1, 6 However, the treatment of choice is endobronchial resection for which there are several options such as mechanical debulking, LASER, electrocautery, argon plasma coagulation and cryotherapy. Surgery is rarely necessary and is usually an option when endobronchial resection is difficult or when pathological findings are controversial.1
Awareness regarding this rare lesion and its endobronchial management can aid in accurately establishing the diagnosis and avoid invasive surgical interventions.7
Conflict of interestThe authors have no conflicts of interest to declare.
Corresponding author. raquel.mendes@CHVNG.MIN-SAUDE.PT


