




In many obstructive airway diseases, the abnormal pulmonary function, with impaired distribution of ventilation and consecutive gas exchange disturbance, limits aerobic working capacity and maximal oxygen consumption (VO2max).1 With regard to pulmonary function and VO2max importance in athletic performance,2 as well as to the close relationship between these two variables, we here report on the causality between dynamic volumes of pulmonary function and maximal oxygen uptake, measured in young elite athletes and their age- and psychometric-matched controls. The study included 45 Caucasian men, all nonsmokers with no history of cardiovascular and respiratory diseases, equally divided into three groups: group A (15 elite aerobic football players (23.7±4.4 years)), group B (15 elite anaerobic karate players (23.8±3.5 years)), group C (15 sedentary controls (23.8±1.7 years)). The research protocol was approved by the local ethical committee and complied with the guidelines of the Declaration of Helsinki.
All participants gave informed written consent before their inclusion. Each subject underwent two protocol measurements: an incremental exercise test on treadmill for VO2max measurement and spirometry tests for the measurement of the pulmonary function: vital capacity – VC, forced vital capacity – FVC, forced expiratory volume in the first second – FEV1 (all presented in percent predicted and as measured values both in liters and percentages); Peak Expiratory Flow – PEF (shown in liters per second) and FEV1/FVC (as percentage). Spirometry was performed using standard spirometer (Turnaic, Pneumotach) Pony FX (Cosmed Pulmonary Function Equipment, Italy). Bruce treadmill protocol (T200; COSMED Ltd, Rome, Italy with Jaeger, Oxycon pro, Wurzburg, Germany) was the standard exercise protocol for this study.3 The duration of the test, measured in seconds and limited by the subject's heart rate, was 12.81 (1.19), 14.53 (2.90) and 15.87 (3.23) for controls, football players and karate players, respectively.
The test was interrupted if any of the following parameters were achieved: age-predicted maximal heart rate; oxygen consumption plateau; respiratory coefficient (RQ) >1.2 and because of any subjective reason. Kruskal–Wallis one way ANOVA test was used to determine differences between groups in relation to measured parameters; Mann–Whitney test was used for inter-group differences. Correlation between dynamic volumes and VO2max was determined by Pearson coefficient. The level of significance was set at 95% for all statistical analyses.
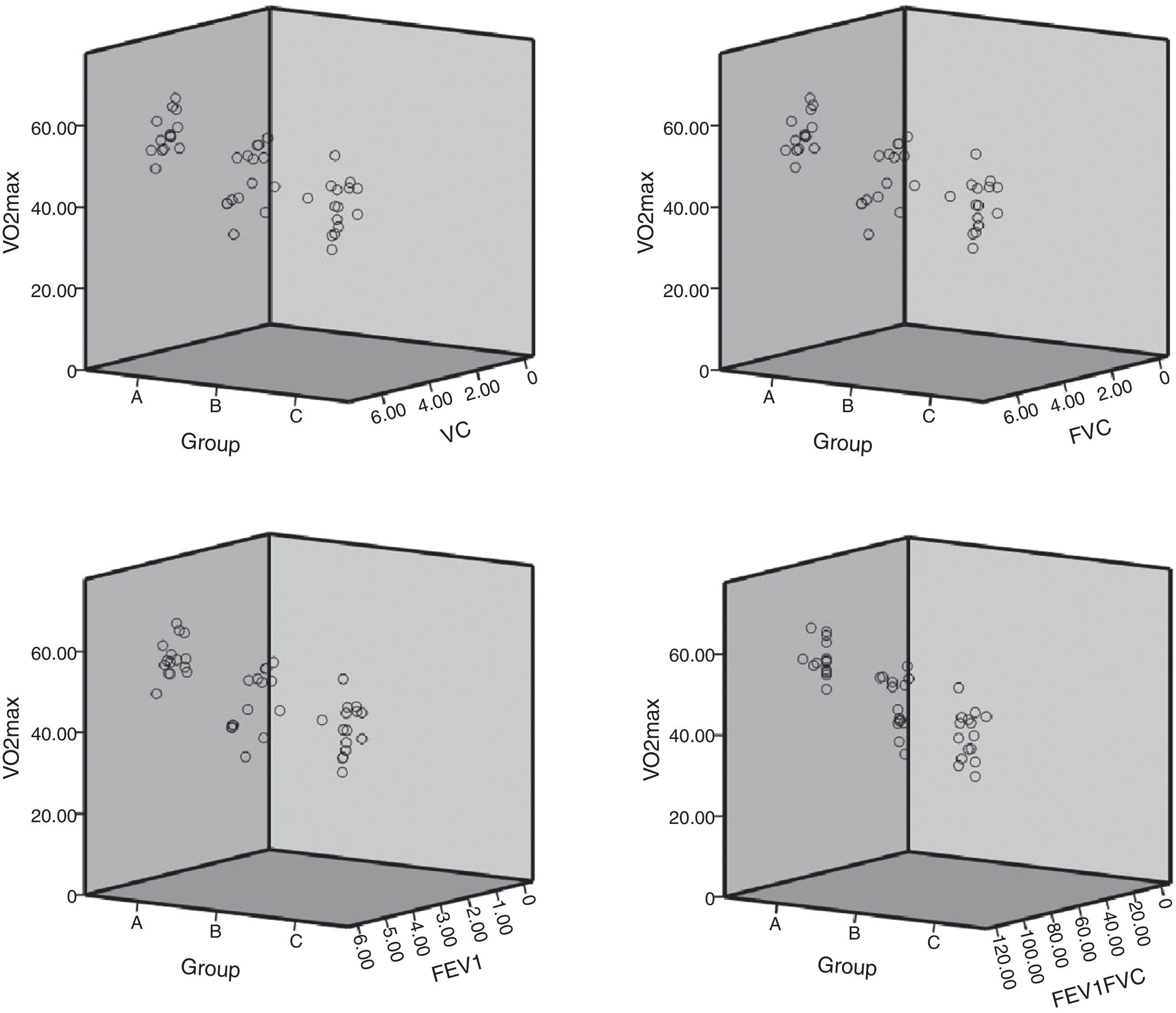
There were no significant differences for any of the pulmonary function measures among athletes. Significant differences were found in VC, FVC, FEV1, FEV1/FVC between aerobics and controls, as well as in PEF (%). Also, higher FEV1, FEV1/FVC and PEF were found in anaerobics than in controls. Statistical difference was observed in percentage of VC, FVC and PEF (%) between groups B and C. As expected, group A had the highest reached value of VO2 max, which proved to be statistically significant as compared to both groups B and C, the latter two showing no significant differences between them (Table 1). No significant correlations were found between VO2max and VC, FVC, FEV1 and FEV1/FVC in any of the investigated groups, although there were noticeable differences in those parameters among them (Fig. 1).
Pulmonary and cardiac parameters for aerobics (A), anaerobics (B) and controls (C).
| Group | Mean (SD) | p† | p†† | ||||
|---|---|---|---|---|---|---|---|
| A | B | C | A/B/C | A vs B | A vs C | B vs C | |
| Pulmonary parameters | |||||||
| Predicted | |||||||
| VC | 5.82 (0.33) | 5.96 (0.68) | 5.57 (0.17) | ns | |||
| FVC | 5.58 (0.31) | 5.78 (0.69) | 5.47 (0.55) | ns | |||
| FEV1 | 4.68 (0.25) | 4.79 (0.58) | 4.71 (0.31) | ns | |||
| PEF | 10.35 (0.37) | 10.77 (1.44) | 11.97 (0.97) | 0.000** | ns | 0.000** | 0.004** |
| Measured (L) | |||||||
| VC | 6.14 (0.37) | 6.04 (0.66) | 5.62 (0.51) | 0.017* | ns | 0.002** | ns |
| FVC | 6.11 (0.37) | 5.89 (0.73) | 5.37 (0.49) | 0.001** | ns | 0.000** | ns |
| FEV1 | 5.03 (0.34) | 4.98 (0.58) | 4.48 (0.35) | 0.002** | ns | 0.000** | 0.018* |
| %FEV1/VC | 93.93 (5.41) | 95.86 (6.02) | 102.11 (5.97) | 0.002** | ns | 0.002** | 0.004** |
| PEF | 10.58 (1.63) | 10.96 (1.04) | 10.08 (0.51) | 0.044* | ns | ns | 0.018* |
| Measured (%) | |||||||
| VC | 105.27 (6.76) | 106.87 (9.29) | 98.80 (6.34) | 0.011* | ns | 0.006** | 0.015* |
| FVC | 109.80 (7.15) | 111.07 (9.76) | 101.87 (5.54) | 0.003** | ns | 0.002** | 0.005** |
| FEV1 | 107.47 (6.53) | 110.40 (12.71) | 105.13 (8.48) | ns | |||
| FEV1/VC | 82.14 (5.06) | 84.08 (4.60) | 81.97 (9.82) | ns | |||
| PEF | 102.53 (17.75) | 111.07 (13.18) | 118.67 (7.96) | 0.001** | ns | 0.000** | 0.046* |
| Cardiac parameters | |||||||
| VO2max | |||||||
| 57.71 (4.41) | 48.98 (6.79) | 44.13 (6.04) | 0.000** | 0.001** | 0.000** | ns | |
VC, vital capacity; FVC, forced vital capacity; FEV1, forced expiratory volume in1 second; PEF, peak expiratoy flow; VC, vital capacity; FEV1/VC-Tiffeneau-Pinelli index; PEF, peek expiratory flow.
The results of the present study have clearly shown positive connection between exercise and both pulmonary and cardiac function. Lung volumes in athletes are disputable and according to some studies depend on the type of sport.4,5 Our previous experiments have shown higher lung volumes in almost all athletes as compared to non-athletes,6,7 which was also confirmed by the current study-higher lung volumes were observed in athletes than in sedentary controls. Physical training improves aerobic capacity. According to a number of studies, VO2max can be increased by 20–30% with 8–10 weeks of training, and 40–50% with one to four years.4,5,8 Indeed, according to our study, athletes (both groups) had higher VO2max than the control group.
The absence of correlation between pulmonary parameters and maximal oxygen uptake in elite athletes is the most noticeable finding of our research. It is in contrast to previously reported study claiming relationship between pulmonary function and VO2max for various sport disciplines,8 finding that subjects with higher VO2max have lower airway resistance. From this point of view it comes to the same thing, since athletes have higher VO2max due to their regular system of training, with a lower incidence of airway resistance coming as a consequence. We should take into account difficulties in distinguishing between exercise-induced bronchospasm and bronchospasm caused by cold or dry air inhalation or previously unrecognized asthma. In mild asthma, exercise is the only cause of asthmatic symptoms sometimes.9 All pulmonary parameters not affecting VO2 max were normal in all of the investigated subjects.
In conclusion, exercise training improves the subject's pulmonary function and VO2max. VO2max is most improved by aerobic type of training; there were no observed differences with regard to respiratory parameters.
Conflicts of interestThe authors have no conflicts of interest to declare.


