

Catathrenia is a rare, idiopathic sleep disorder classified as an isolated symptom of sleep-disordered breathing (SDB).1 Its prevalence is unknown,2 and its onset is usually in adolescence.3 Affected individuals are frequently unaware of their problem, and family members or bed partners commonly report strange sounds while breathing during sleep.1,3
The hallmark of this disorder is a deep inspiration followed by prolonged expiration and a monotonous vocalization resembling groaning, usually during rapid eye movement sleep.1
No pharmacological treatments are available,4 but some studies have shown partial or complete resolution of events with continuous positive airway pressure (CPAP) therapy, especially in patients with a SDB associated.2,4,5
The purpose of this study was to assess the effectiveness of CPAP treatment and a 6-month CPAP therapy in patients with catathrenia without SDB events associated.
We performed a prospective study of patients with catathrenia, diagnosed between 2008 and 2014, who underwent a CPAP titration PSG and subsequently initiated home CPAP therapy for 6 months. There were no exclusion criteria.
During anamnesis, the evaluated symptoms were: groaning, snoring, choking, apnea, daytime sleepiness (Epworth Sleepiness Scale [ESS]), headache, fatigue, and anxiety/depression. The diagnosis was based on an overnight polysomnogram (PSG). A catathrenia event was defined as a deep inhalation followed by prolonged exhalation, and a monotonous vocalization resembling groaning.1 After the diagnostic study, patients underwent a CPAP titration PSG to correct catathrenia events. CPAP began at 4cmH2O and was progressively increased according to the type of respiratory events observed. In the presence of obstructive events, such as obstructive apnea or hypopnea, the pressure was increased by 2cmH2O every 15min, and in the presence of snoring, respiratory effort-related arousals, and/or groaning episodes, it was increased by 1 cmH2O every 15min, until the events reduced in number or disappeared. Once the optimal pressure was achieved, CPAP was initiated at home with the established pressure. The patients were evaluated at 1 and 3 months of CPAP therapy, in the presence of their bed partner. During the evaluation, patients were questioned how they would classify their daytime complaints improvement (scale 0–100). After the first 3 months of CPAP therapy, they were contacted monthly by telephone to evaluate improvements over the remaining 3 months of therapy.
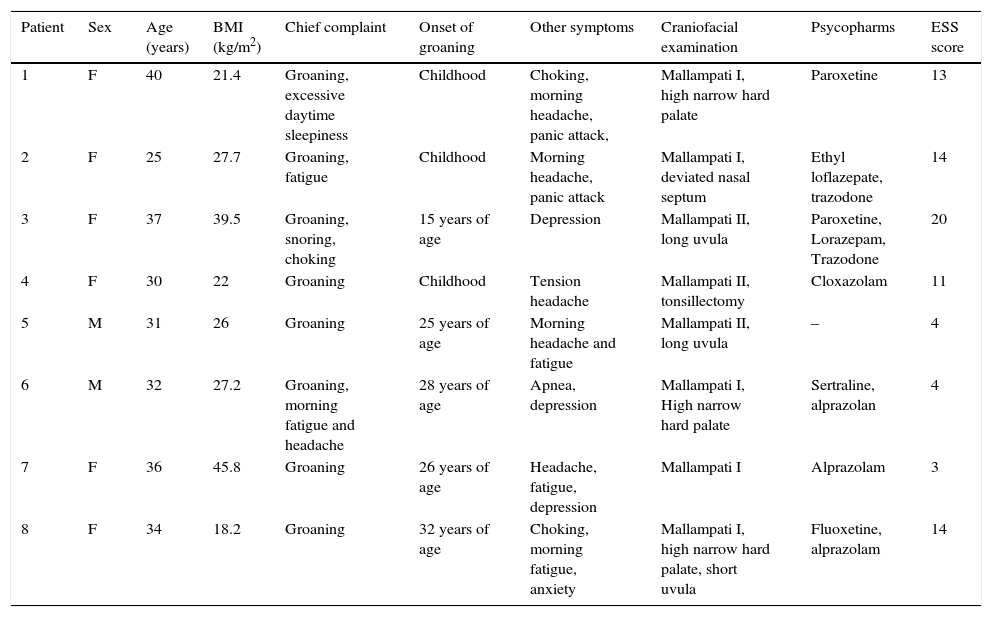
Eight patients were included. Five patients had abnormal sleepiness (ESS>10). Six patients had symptoms of anxiety disorder and 7 were medicated with psycopharms (Table 1).
Demographic and clinical characteristics of patients.
| Patient | Sex | Age (years) | BMI (kg/m2) | Chief complaint | Onset of groaning | Other symptoms | Craniofacial examination | Psycopharms | ESS score |
|---|---|---|---|---|---|---|---|---|---|
| 1 | F | 40 | 21.4 | Groaning, excessive daytime sleepiness | Childhood | Choking, morning headache, panic attack, | Mallampati I, high narrow hard palate | Paroxetine | 13 |
| 2 | F | 25 | 27.7 | Groaning, fatigue | Childhood | Morning headache, panic attack | Mallampati I, deviated nasal septum | Ethyl loflazepate, trazodone | 14 |
| 3 | F | 37 | 39.5 | Groaning, snoring, choking | 15 years of age | Depression | Mallampati II, long uvula | Paroxetine, Lorazepam, Trazodone | 20 |
| 4 | F | 30 | 22 | Groaning | Childhood | Tension headache | Mallampati II, tonsillectomy | Cloxazolam | 11 |
| 5 | M | 31 | 26 | Groaning | 25 years of age | Morning headache and fatigue | Mallampati II, long uvula | – | 4 |
| 6 | M | 32 | 27.2 | Groaning, morning fatigue and headache | 28 years of age | Apnea, depression | Mallampati I, High narrow hard palate | Sertraline, alprazolan | 4 |
| 7 | F | 36 | 45.8 | Groaning | 26 years of age | Headache, fatigue, depression | Mallampati I | Alprazolam | 3 |
| 8 | F | 34 | 18.2 | Groaning | 32 years of age | Choking, morning fatigue, anxiety | Mallampati I, high narrow hard palate, short uvula | Fluoxetine, alprazolam | 14 |
F – female; M – male; BMI – body mass index; ESS – Epworth Sleepiness Scale.
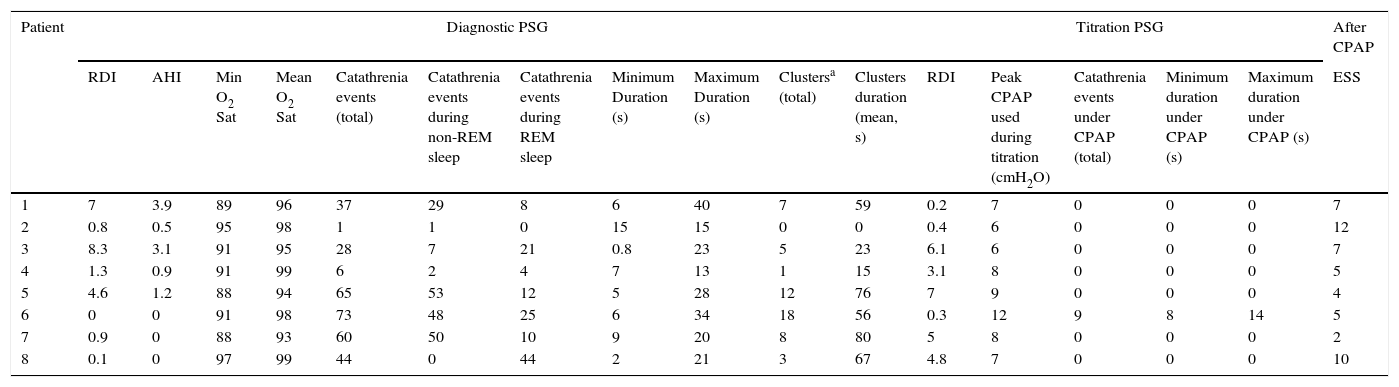
Catathrenia events during the diagnostic and CPAP titration polysomnograms are displayed on Table 2. Diagnostic PSG showed a mean respiratory disturbance index (RDI) of 2.8±3.29 events/h, a mean apnea–hypopnea index of 1.2±1.5 events/h. The mean number of catathrenia events was 39.3±26.6. Patient #6 experienced a partial resolution of events, despite an increase in pressure up to 12cmH2O. This patient did not tolerate a higher pressure.
Catathrenia events and sleep characterization during the diagnostic PSG.
| Patient | Diagnostic PSG | Titration PSG | After CPAP | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| RDI | AHI | Min O2 Sat | Mean O2 Sat | Catathrenia events (total) | Catathrenia events during non-REM sleep | Catathrenia events during REM sleep | Minimum Duration (s) | Maximum Duration (s) | Clustersa (total) | Clusters duration (mean, s) | RDI | Peak CPAP used during titration (cmH2O) | Catathrenia events under CPAP (total) | Minimum duration under CPAP (s) | Maximum duration under CPAP (s) | ESS | |
| 1 | 7 | 3.9 | 89 | 96 | 37 | 29 | 8 | 6 | 40 | 7 | 59 | 0.2 | 7 | 0 | 0 | 0 | 7 |
| 2 | 0.8 | 0.5 | 95 | 98 | 1 | 1 | 0 | 15 | 15 | 0 | 0 | 0.4 | 6 | 0 | 0 | 0 | 12 |
| 3 | 8.3 | 3.1 | 91 | 95 | 28 | 7 | 21 | 0.8 | 23 | 5 | 23 | 6.1 | 6 | 0 | 0 | 0 | 7 |
| 4 | 1.3 | 0.9 | 91 | 99 | 6 | 2 | 4 | 7 | 13 | 1 | 15 | 3.1 | 8 | 0 | 0 | 0 | 5 |
| 5 | 4.6 | 1.2 | 88 | 94 | 65 | 53 | 12 | 5 | 28 | 12 | 76 | 7 | 9 | 0 | 0 | 0 | 4 |
| 6 | 0 | 0 | 91 | 98 | 73 | 48 | 25 | 6 | 34 | 18 | 56 | 0.3 | 12 | 9 | 8 | 14 | 5 |
| 7 | 0.9 | 0 | 88 | 93 | 60 | 50 | 10 | 9 | 20 | 8 | 80 | 5 | 8 | 0 | 0 | 0 | 2 |
| 8 | 0.1 | 0 | 97 | 99 | 44 | 0 | 44 | 2 | 21 | 3 | 67 | 4.8 | 7 | 0 | 0 | 0 | 10 |
PSG – polysomnogram; CPAP – continuous positive airway pressure; RDI – respiratory disturbance index; AHI – apnea/hypopnea index; TST – total sleep time; REM – rapid eye movement; NREM – non rapid eye movement; N1, N2, N3 – sleep stages of NREM.
After 1 month of therapy, seven patients had significantly fewer moaning/groaning episodes and patient #6 reported a moderate reduction. After 3 months, seven patients reported complete resolution of nocturnal episodes and patient #6 reported maintenance of the moderate reduction achieved with the first month of therapy. An improvement in daytime complaints was reported by all patients (mean subjective improvement of 80/100). One patient maintained an abnormal sleepiness (ESS>10). Complete resolution of events was maintained during the 6 months of follow-up, except for patient #6 who continued to exhibit partial improvement. This patient was subsequently treated with clonazepam for 6 months, but showed no additional improvements.
Although CPAP titration has been used in previous studies of catathrenia, its goal was to correct apnea, hypopnea, and flow limitation.2,5 Other studies have reported an improvement in moaning/groaning with CPAP, but the majority of patients had associated SDB.2,4
Iriarte et al.6 have argued that the pathological mechanism underlying catathrenia is mainly obstructive. Our results support this theory, as our patients responded to positive airway pressure. Vetrugno et al.3 described a series of 10 patients with catathrenia and a normal RDI (as our patients) who had a post-inspiratory positive rise in endoesophageal pressure during events, higher than that observed in expiration in eupnoic breathing, suggesting an expiratory upper airway obstruction. One possible mechanism that might explain the response observed in our patients is subtotal closure of the glottis during expiration.3
Our patients presented some differences in relation to previous published series: there was a preponderance of women; OSA was absent and the majority of patients were sleepy. It is possible that patients with more severe SDB, catathrenia events were unnoticed or obscured by other respiratory sounds and therefore not detected. This may explain the lower prevalence in men and patients with OSA in our series. The higher frequency of young women is also probably related to the less severe SDB. As for sleepiness, it may be argued that it may be related to the concomitant psychiatric disorders and medications. Other sleepiness causes, recognized to contribute to sleep deprivation, were not analyzed in the present study. However, its improvement following efficacious catathrenia treatment suggest an association between both complaints and warrants further research. While no clear association has been demonstrated between catathrenia and psychiatric disorders,1 they marked a bold presence in our study (7/8 patients). Examination by a psychiatric specialist with validated questionnaires would have provided a clearer idea of the presence of psychiatric disease in our patients. We believe CPAP treatment in patients with catathrenia without SDB events can improve nocturnal groaning episodes and daytime complaints. In a future research, laryngoscopy during sleep may help to elucidate catathrenia pathophysiology.7
Conflicts of interestThe authors have no conflicts of interest to declare.


