

Tuberculosis (TB) remains a major global public health problem and is the second leading cause of death from infectious disease worldwide.1
Delays in diagnosis may worsen the disease, increase the risk of death and enhance TB transmission within the community. These delays may be attributed to both patients and the health care system.3
This study was designed to assess risk factors associated with an increased time between symptoms and diagnosis.
A cross-sectional study involved 68 patients identified by passive screening and being treated for TB at a TB outpatient clinic, in Gaia, Portugal between November 2013 and April 2014. Each patient answered a semi-structured questionnaire on the day of clinical appointment. The questionnaire was designed to assess patient progress from initial symptoms until diagnosis.
Of the 68 patients, 40 (58.8%) were male, with mean age 47.1 years. Twenty patients (29.4%) presented with respiratory symptoms, 31 (45.6%) with systemic symptoms and 17 (25%), with both. Of these 68 patients, 23 (33.8%) were unemployed. The first health unit identified was: for 36 patients (52.9%) the hospital emergency room, for 32 patients (47.1%) the primary care physician, a private clinic or TB outpatient clinic. Thirty-seven (54.4%) required 1–2 visits to health facilities before diagnosis, and 31 (45.6%) required more than 2 visits (Table 1).
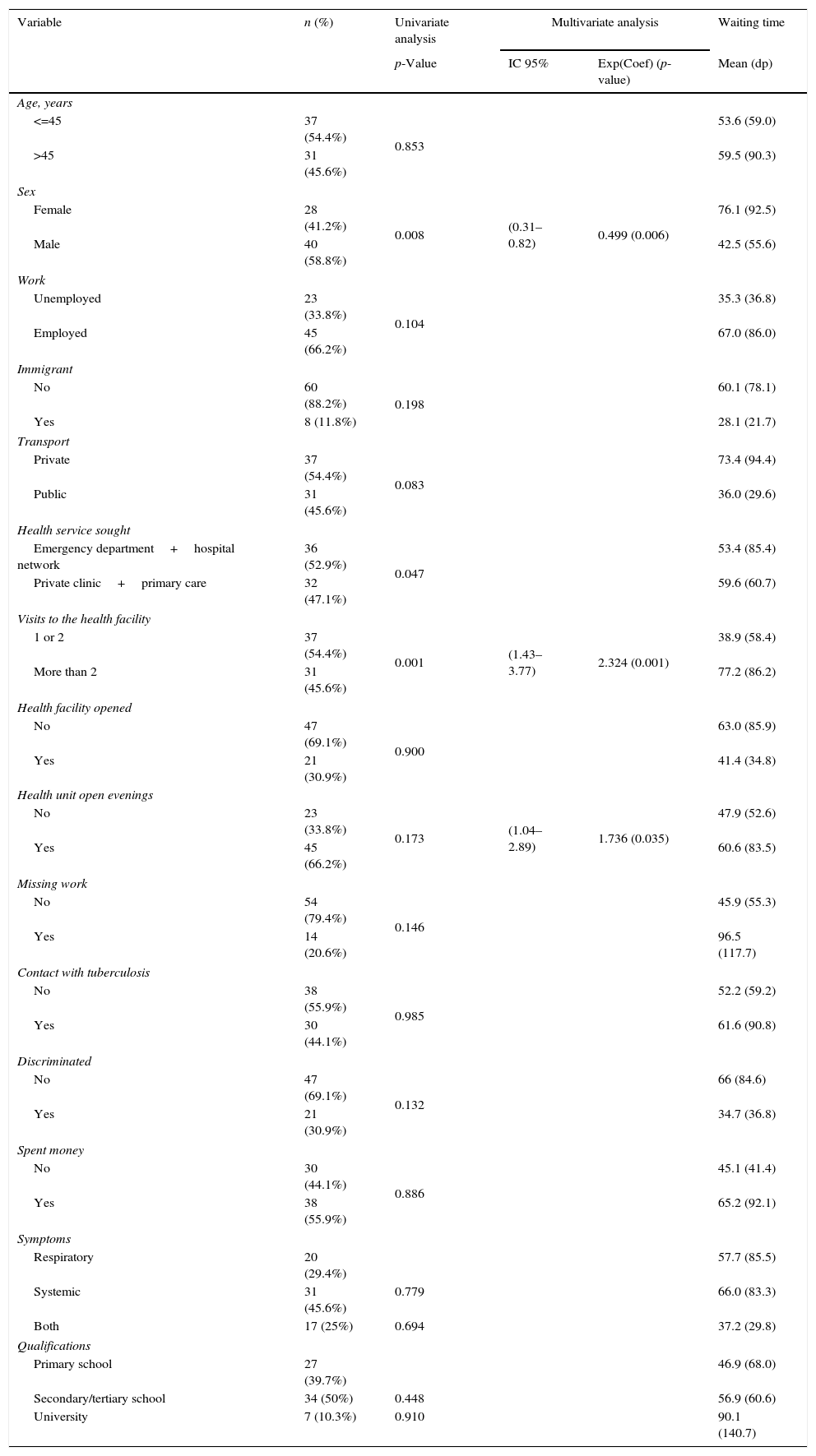
Risk factors associated with increased waiting time for TB diagnosis.
| Variable | n (%) | Univariate analysis | Multivariate analysis | Waiting time | |
|---|---|---|---|---|---|
| p-Value | IC 95% | Exp(Coef) (p-value) | Mean (dp) | ||
| Age, years | |||||
| <=45 | 37 (54.4%) | 0.853 | 53.6 (59.0) | ||
| >45 | 31 (45.6%) | 59.5 (90.3) | |||
| Sex | |||||
| Female | 28 (41.2%) | 0.008 | (0.31–0.82) | 0.499 (0.006) | 76.1 (92.5) |
| Male | 40 (58.8%) | 42.5 (55.6) | |||
| Work | |||||
| Unemployed | 23 (33.8%) | 0.104 | 35.3 (36.8) | ||
| Employed | 45 (66.2%) | 67.0 (86.0) | |||
| Immigrant | |||||
| No | 60 (88.2%) | 0.198 | 60.1 (78.1) | ||
| Yes | 8 (11.8%) | 28.1 (21.7) | |||
| Transport | |||||
| Private | 37 (54.4%) | 0.083 | 73.4 (94.4) | ||
| Public | 31 (45.6%) | 36.0 (29.6) | |||
| Health service sought | |||||
| Emergency department+hospital network | 36 (52.9%) | 0.047 | 53.4 (85.4) | ||
| Private clinic+primary care | 32 (47.1%) | 59.6 (60.7) | |||
| Visits to the health facility | |||||
| 1 or 2 | 37 (54.4%) | 0.001 | (1.43–3.77) | 2.324 (0.001) | 38.9 (58.4) |
| More than 2 | 31 (45.6%) | 77.2 (86.2) | |||
| Health facility opened | |||||
| No | 47 (69.1%) | 0.900 | 63.0 (85.9) | ||
| Yes | 21 (30.9%) | 41.4 (34.8) | |||
| Health unit open evenings | |||||
| No | 23 (33.8%) | 0.173 | (1.04–2.89) | 1.736 (0.035) | 47.9 (52.6) |
| Yes | 45 (66.2%) | 60.6 (83.5) | |||
| Missing work | |||||
| No | 54 (79.4%) | 0.146 | 45.9 (55.3) | ||
| Yes | 14 (20.6%) | 96.5 (117.7) | |||
| Contact with tuberculosis | |||||
| No | 38 (55.9%) | 0.985 | 52.2 (59.2) | ||
| Yes | 30 (44.1%) | 61.6 (90.8) | |||
| Discriminated | |||||
| No | 47 (69.1%) | 0.132 | 66 (84.6) | ||
| Yes | 21 (30.9%) | 34.7 (36.8) | |||
| Spent money | |||||
| No | 30 (44.1%) | 0.886 | 45.1 (41.4) | ||
| Yes | 38 (55.9%) | 65.2 (92.1) | |||
| Symptoms | |||||
| Respiratory | 20 (29.4%) | 57.7 (85.5) | |||
| Systemic | 31 (45.6%) | 0.779 | 66.0 (83.3) | ||
| Both | 17 (25%) | 0.694 | 37.2 (29.8) | ||
| Qualifications | |||||
| Primary school | 27 (39.7%) | 46.9 (68.0) | |||
| Secondary/tertiary school | 34 (50%) | 0.448 | 56.9 (60.6) | ||
| University | 7 (10.3%) | 0.910 | 90.1 (140.7) | ||
The median time from onset of symptoms to diagnosis was 36 days.
Being a woman (waiting time for women 76.1 days vs 42.5 days for men), employed (67.0 vs 35.3 days), native (60.1 vs 28.1 days), having an university degree (90.1 vs 46.9 days) and having used private transportation (73.4 vs 36.0 days) to arrive to clinical appointment was associated with a longer waiting time until diagnosis (Table 1).
In the multivariate analysis just being a woman (p=0.006), and visiting the health unit after 18:00h (p=0.035) was significantly associated to a longer waiting period (Table 1).
The median waiting time from symptoms to diagnosis in our population was shorter than in other studies. A previous study in Portugal reported a median waiting time of 92 days4 while among low and median income countries, median total delay ranged from 25 days in China to 185 days in Tanzania, with an average of 67.8 days.3 Among high income countries, delays ranged from 42 days in Japan to 89 days in USA, with an average of 61.3 days.3
The waiting time from symptom detection to diagnosis was twice as long for women than for men. As there is a greater proportion of the disease in men,2 this may cause lower degree of suspicion in women.
Ability to attend health facilities after 18h was associated with longer period to diagnosis. This was unexpected, as we hypothesized that increased hours of operation would be associated with easier access to health care and a more rapid diagnosis. During evening hours, however, these units function as emergency units, with no scheduled appointments, and with patients being seen by different medical doctors at each visit. Moreover, these units may lack appropriate diagnostic resources and may be limited in terms of scheduling appropriate patient follow up. In fact, 45.6% of the patients required more than 2 clinical appointments before diagnosis.
Access to care can depend on a complex interaction of multiple factors including awareness even in unknown risk groups; the responsiveness of units to the needs of users, including availability, accessibility, affordability, appropriateness and acceptability; and patient behavior seeking health care, which may be influenced by socio-cultural, behavioral, financial and organizational factors.5
Although there are some known risk factors associated with TB, still the great majority does not have any. In our population, patients with a characteristic usually associated with a better social status were the ones with a longer waiting period until diagnosis.
Being a woman was the only significant characteristic associated to the patient; attending health facilities without any follow up was associated with longer period to diagnosis.
Awareness of TB should be enhanced.
Authors’ contributionRaquel Duarte and Marta Guimarães devised the study. Marta Guimarães worked up the draft manuscript. Marta Guimarães and Olena Oliveira collected the data. Raquel Duarte revised the draft.
Conflicts of interestThe authors have no conflicts of interest to declare.


