

Diabetes mellitus (DM) is a risk factor for tuberculosis (TB) and may modify its presenting features.
The aim of this study was to find out the influence of DM on clinical, radiological and treatment features of TB in hospitalized patients.
Material and methodsIn a retrospective study we reviewed the records of 123 patients with TB and DM admitted from 2000 to 2008 and compared this group with another one of 123 patients with TB without DM.
ResultsAlthough in both groups multilobar lung lesions predominated, there were more cases of isolated lower lung field (LLF) involvement in diabetics than in nondiabetics (10.6% vs 3.3%, p=0.03). Cavitary lesions were less frequent (63.4% vs 82.1%, p=0.01) and extra-pulmonary TB manifestations were more frequent (28.5% vs 16.3%, p=0.02) in diabetics than in nondiabetics. There were no significant differences between groups regarding multidrug resistant – TB (MDR-TB) and adverse effects of anti-tuberculosis drugs. The in-hospital mortality was higher in diabetics (8.1% vs 0.8%, p=0.01), but using a binary logistic regression there was significant difference in mortality only in respect to the variable MDR-TB.
ConclusionsThis study showed that DM affected some clinical and radiological presenting features in hospitalized TB patients. LLF involvement and extra-pulmonary TB manifestations were more frequent in diabetic patients than in nondiabetic ones.
A diabetes mellitus (DM) é um fator de risco para a tuberculose (TB) e pode modificar a sua forma de apresentação.
O objetivo deste estudo foi o de compreender a influência da DM nos aspetos clínicos, imagiológicos e de tratamento da TB em doentes hospitalizados.
Material e MétodosNum estudo retrospetivo, revimos os processos clínicos de 123 doentes com TB e DM, internados entre 2000 e 2008. Este grupo foi comparado com outro constituído por 123 doentes com TB e sem DM.
ResultadosApesar de em ambos os grupos ter predominado o envolvimento pulmonar multilobar, registaram-se mais casos de envolvimento isolado dos campos pulmonares inferiores nos diabéticos do que nos não diabéticos (10,6% vs 3,3%, p=0,03). As lesões cavitadas foram menos frequentes (63,4% vs 82,1%, p=0,01) e as manifestações extrapulmonares da TB mais frequentes (28,5% vs 16,3%, p=0,02) nos diabéticos, comparativamente com os não diabéticos. Não se registaram diferenças estatisticamente significativas entre os dois grupos no que concerne ao diagnóstico de TB multirresistente (MDR-TB) e ao surgimento de efeitos adversos da terapêutica antibacilar. A mortalidade intra-hospitalar foi superior nos diabéticos (8,1% vs 0,8%, p=0,01). No entanto, utilizando a regressão logística binária, só houve diferença estatisticamente significativa na mortalidade em relação à variável MDR-TB.
ConclusãoEste estudo mostrou que a DM pode alterar alguns aspetos clínicos e imagiológicos da forma de apresentação da TB em doentes hospitalizados. O envolvimento isolado dos campos pulmonares inferiores e as manifestações extrapulmonares da TB foram mais frequentes nos diabéticos do que nos não diabéticos.
Over the past decades, tuberculosis (TB) incidence has declined in some developed countries, but has risen in countries with high rates of infection with human immunodeficiency virus (HIV).1
Diabetes mellitus (DM) is currently an important chronic disease mainly in developed countries. In developing countries the prevalence of DM is also soaring.1
Susruta, an Indian physician (600 A.D.), was probably the first to note the association between TB and DM.2
Many studies have shown that the prevalence of TB among diabetics, especially in those with poor glycemic control, is higher than in nondiabetic population.1,3 In some case-control studies the authors concluded that the relative odds of developing TB were higher (ranging from 2.44 to 8.33) in diabetic patients than in nondiabetics.1
DM causes dysfunction of the immune system, which can increase the susceptibility to TB. The main immunologic abnormalities are: abnormal functions of polymorphonuclear cells, decreased peripheral monocytes with impaired phagocytosis, poor blast transformation of lymphocytes and defect in complement opsonic function. The pulmonary physiologic functions are also altered in diabetic patients.2
At the same time, TB may increase the blood glucose levels and trigger a “latent diabetes” or be a factor in its decompensation. Fever, inactivity and malnutrition stimulate the stress hormones which raise the blood sugar level. Plasma levels of interleukin-1 and tumor necrosis factor-alpha are raised in severe TB, which can stimulate the anti-insulin hormones. The antituberculosis (anti-TB) drugs also influence the glycemic control. Rifampicin, as an inducer of the hepatic microsomal enzyme system, increases metabolism of sulphonylureas and biguanides.2,4 Conversely, DM can have a negative effect on TB treatment because hyperglycemia lowers the bioavailability of rifampicin.4 Pyrazinamide may cause hypoglycemia with difficulty in controlling blood sugar levels.2,5
DM is known to modify the clinical features of pulmonary TB.6 DM has been associated with increased risk of TB treatment failure or relapse and of increased risk of mortality.1
The radiographic patterns of TB in diabetic patients may also be different from those found in nondiabetics, as was initially reported by Sosman and Steidl. These authors found a higher rate of lower lung field (LLF) involvement in their diabetic patients.7
The aim of this study was to find out the influence of DM on clinical, radiological and treatment features of TB in hospitalized patients.
Material and methodsThis retrospective study was conducted at the Respiratory Department of Centro Hospitalar Lisboa Norte – Hospital Pulido Valente. We reviewed all records (123) of patients with a discharge diagnosis of pulmonary TB and DM admitted from 2000 to 2008 and compared this group with a control group of 123 patients with pulmonary TB without DM. The control group was randomly selected from a database of TB patients without DM admitted in the same period.
Patients with HIV infection were excluded from both groups. Patients with cancer were not excluded; however, none of them were under chemotherapy or radiotherapy. There were no patients under other immunosuppressive therapies prior to admission.
Patients were included in the DM group if they had a previous history of DM and had been receiving insulin and/or an oral hypoglycemic agent at the time of hospital admission or were found to have two or more fasting blood glucose levels greater than 126mg/dl during hospital stay.
Reviewed parametersUpon examination of the records, the following parameters were compared between the two groups of patients: age, gender, immigration, lung lesions location, cavitary lesions, extra-pulmonary TB manifestations, multidrug-resistant TB (MDR-TB), adverse effects of anti-TB drugs, length of hospital stay and in-hospital mortality.
Radiographic interpretationThe radiographic findings were collected using the chest roentgenograms (view posteroanterior) obtained in all patients at the time of diagnosis and the chest computed tomography (CT) scans made in about 30% of the patients in each group. The chest roentgenograms and the chest CT scans were read by two of the investigators.
We considered three possible radiographic distributions of the lung lesions: isolated lower lung field (LLF) involvement, isolated upper lung field (ULF) involvement and multilobar involvement. In posteroanterior roentgenograms, LLF was defined as the area below an imaginary line traced across the hila and including the parahilar region.
AnalysisStatistical analysis was performed using SPSS (Statistical Package for the Social Sciences) version 15.0. Statistical differences between groups were evaluated using the T-test, Chi-square and binary logistic regression (significance level p<0.05).
Ethical approval was not required.
ResultsNinety-nine patients (80.5%) in the study group had prior diagnosis of DM and in 24 (19.5%) cases the diagnosis was confirmed during the admission (13 patients reported having DM but were not taking antidiabetic drugs at the time of admission and the remaining 11 were unaware of having DM). From the 99 patients who had been diagnosed with DM prior to admission, 74 were treated with oral antidiabetic drugs and 25 with insulin. During hospital stay, 78 patients (63.4%) were treated with insulin, 41 (33.3%) were on oral antidiabetic drugs and 4 (3.3%) were diet controlled.
The mean age of patients in the diabetic group was 59.2±14.4 years, while in the nondiabetic group it was 41.4±13.8 years. Although diabetics tend to be older, the difference was not statistically significant.
There were 87 males (70.7%) in the diabetic group and 86 (69.9%) in the nondiabetic group. The difference was not statistically significant.
The nondiabetic group had 38 immigrants (30.9%) while the diabetic group had 19 (15.5%). This difference was statistically significant (p=0.04). The immigrants were mainly from African countries.
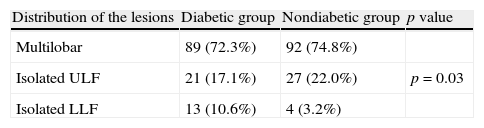
The two groups showed different radiographic distribution of the lesions (Table 1). In both groups multilobar lesions predominated, but there were significantly more cases of isolated LLF involvement in diabetic patients than in nondiabetics (10.6% vs 3.3%, p=0.03).
Cavitary lesions were present in 101 patients (82.1%) of the nondiabetic group and in 78 patients (63.4%) of the diabetic group. This difference was statistically significant (p=0.01).
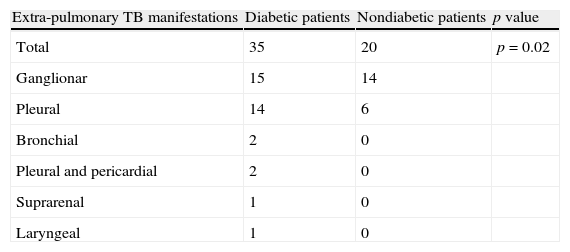
Extra-pulmonary manifestations were present in 35 diabetic patients (28.5%) and in 20 nondiabetic patients (16.3%). This difference was also statistically significant (p=0.02). The extra-pulmonary manifestations are presented in Table 2.
The diagnosis of MDR-TB was made in 5 patients (4.1%) of the diabetic group and from those, 2 cases were extensively drug-resistant TB (XDR-TB). In the nondiabetic group there were 6 patients (4.9%) with MDR-TB and from those, 4 patients had XDR-TB. The difference between the two groups was not statistically significant.
There were 13 cases (10.6%) of adverse reactions to anti-TB drugs in the diabetic group and 15 cases (12.2%) in the nondiabetic group. There was no significant difference between the two groups. In the diabetic group the adverse reactions to anti-TB drugs were: hepatic (4 cases), gastrointestinal (4 cases), renal (2 cases) and others (3 cases).
The length of hospital stay was similar in both groups (diabetic group: 25.7±20.7 days; nondiabetic group: 25.6±22.5 days).
The in-hospital mortality rate was 8.1% (10 patients) in the group of diabetics and 0.8% (1 patient) in nondiabetics. The difference between the two groups was statistically significant (p=0.01). In the diabetic group, 6 out of 10 patients died from causes mainly related with TB. The causes of death in the other 4 diabetic patients were: advanced lung cancer (2 patients), pulmonary embolism (1 patient) and stroke (1 patient). The cause of death of the nondiabetic patient was directly related with TB.
With regard to mortality, we carried out a binary logistic regression with the following dependent variables: age, DM diagnosis, lung lesions location, cavitary lesions, extra-pulmonary TB manifestations, MDR-TB and adverse effects of anti-TB drugs. There was significant difference in mortality only in respect to the variable MDR-TB. Patients with MDR-TB had a relative risk of death of 9.47 (95% CI 1.48–60.6), compared to those without MDR-TB. Indeed, 18.2% of patients with MDR-TB died, compared to 3.8% of patients without MDR-TB (p=0.02).
We also compared the group of 99 patients who were taking antidiabetic drugs before the admission with the group of 24 patients who were not, concerning the following parameters: lung lesions location, cavitary lesions, extra-pulmonary TB manifestations, MDR-TB, adverse effects of anti-TB drugs and in-hospital mortality. We found that the only statistically significant difference was the presence of extrapulmonary manifestations. Patients who were not taking antidiabetic drugs before the admission had extrapulmonary manifestations more frequently (p=0.037).
DiscussionThe main finding of this study was that DM affected the presenting features of TB in hospitalized patients resulting in a higher frequency of extra-pulmonary TB manifestations and of isolated LLF involvement. Diabetic patients also showed a higher in-hospital mortality rate.
Despite being retrospective, the major strengths of this study were the significant size of the sample, the good quality of data collection and the inclusion of a control group. The major limitation was related to the fact that the control group was not perfectly matched with the diabetic group, in what concerns age and ethnicity.
The literature describes three categories on hospitalized patients with hyperglycemia: medical history of diabetes, unrecognized diabetes and hospital-related hyperglycemia. It is important, after discharge, to distinguish between group two and group three. Taking into account that this study was a retrospective one and that the patients were followed in other health institutions after discharge it was impossible to know their glycemic state later. So it was not possible to confirm which of the patients who were unaware of having diabetes prior to admission were actually diabetics or had just hospital-related hyperglycemia. In an attempt to better address this issue, we compared the group of 99 patients who were taking antidiabetic drugs before the admission with the group of 24 patients that were not concerning many parameters. We found that the only statistically significant difference was the presence of extrapulmonary manifestations.
In accordance with some published studies, these data showed higher rate of LLF involvement in the diabetic group than in nondiabetic. In one of the largest series, Aktogu et al. found a higher rate of LLF TB among diabetics as compared with nondiabetics (11% and 5.3%, respectively).8 Singla et al. observed in their study that isolated LLF lesions were significantly more common in diabetic than in nondiabetic patients (23.5% vs 2.4%).6
Pérez-Guzmán et al. showed in their study that the TBDM group had a significantly higher rate of LLF lesions in comparison with the TB group (19% vs 7%).9
In contrast to Singla's6 and Pérez-Guzmán's data,9 where the diabetic group had a significantly higher frequency of cavitary lesions than the nondiabetic group, this study showed a lower frequency of cavitary lesions in the diabetic patients.
Another important clinical feature was the higher rate of extra-pulmonary manifestations in diabetic patients than in nondiabetic ones.
The explanation for both the radiological pattern and high frequency of extra-pulmonary manifestations in diabetic patients can be related to some degree of immunosuppression induced by DM.2 In fact, the clinical and radiological presentation of TB in diabetic patients has some similarities to that seen in HIV infected patients. In this specific group, as the immunity declines, the patients are more likely to have atypical radiographic findings, including non-cavitatory pulmonary infiltrates with no particular preference for the ULF.10,11
Conventionally, it is referred that diabetics have a higher incidence of anti-tuberculosis drugs resistance.12 Zhang et al. observed that a higher rate of MDR-TB among diabetic patients was higher than that among nondiabetics (17.7% vs 8.4%).13 However, in this study, as well as in Singla's, there was no significant difference between diabetics and nondiabetics regarding the diagnosis of MDR-TB.6 These differences have no plausible scientific explanation, justifying more studies about the frequency of MDR-TB in diabetic patients.
There were also no significant differences between the two groups regarding the presence of adverse reactions to anti-TB drugs. There is a paucity of published reports concerning this feature.
We found that the in-hospital mortality rate was significantly higher in diabetic group and deaths were mainly TB related, but using a binary logistic regression there was significant difference in mortality only in respect to the variable MDR-TB. Dooley et al. showed that patients with DM had 2.0 times higher odds of death than patients without DM.1
ConclusionIn conclusion, this study showed that DM affected some clinical and radiological presenting features in hospitalized TB patients. LLF involvement and extra-pulmonary TB manifestations were more frequent in diabetic patients than in nondiabetic ones.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Carreira S, et al. Impacto da diabetes na forma de apresentação da tuberculose em doentes hospitalizados. Rev Port Pneumol. 2012. http://dx.doi.org/10.1016/j.rppneu.2012.04.001.


