

Chronic obstructive pulmonary disease (COPD) is one of the most common chronic diseases and a major cause of morbidity and mortality. An imbalance between oxidants and antioxidants (oxidative stress) has been proposed as a critical event in the pathogenesis of COPD. The increased oxidative stress in patients with COPD is the result of exogenous oxidants namely pollutants and cigarette smoke as well as endogenous oxidant production during inflammation. The aim of the present study was to clarify the hypothesis about the presence of an imbalance between oxidants and the antioxidant defences associated to COPD. In this study, we evaluated a biomarker of oxidative stress (malondialdehyde, a lipid peroxidation derived product) and non-enzymatic antioxidants (vitamin C and the sulphydryl groups) in COPD patients and healthy controls. The marker of oxidative stress was found to be significantly (p<0.001) higher in COPD patients when compared with control group. No age dependent changes in the plasma levels of lipid peroxidation products were found. COPD patients had a significant (p<0.001) decrease in antioxidant status as compared with control group. Our results show that oxidative stress is an important pathophysiologic change in COPD.
A doença pulmonar obstrutiva crónica (DPOC) é uma das doenças crónicas mais comuns e representa uma importante causa de morbilidade e mortalidade. Um desequilíbrio entre oxidantes e antioxidantes (stress oxidativo) tem sido proposto como um acontecimento importante na patogénese da DPOC. O aumento do stress oxidativo em doentes com DPOC é o resultado da presença de oxidantes exógenos, nomeadamente, poluentes e fumo do tabaco, assim como oxidantes endógenos produzidos durante a inflamação. O objetivo do presente estudo consistiu em clarificar a hipótese sobre a existência de um desequilíbrio entre oxidantes e as defesas antioxidantes associado à DPOC. Neste estudo, avaliou-se um biomarcador do stress oxidativo (malonildialdeído, um produto resultante da peroxidação lipídica) e antioxidantes não-enzimáticos (vitamina C e grupos sulfidrilo), em doentes com DPOC e em controlos saudáveis. Observou-se um aumento significativo (p<0,001) do marcador do stress oxidativo nos doentes com DPOC comparativamente ao grupo controlo. Não foram encontradas alterações dependentes da idade nos níveis dos produtos da peroxidação lipídica. Os doentes DPOC apresentaram uma diminuição significativa (p<0,001) do status antioxidante, comparativamente ao grupo controlo. Os nossos resultados evidenciam que o stress oxidativo representa uma importante alteração fisiopatológica na DPOC.
Chronic obstructive pulmonary disease (COPD) is one of the most common chronic diseases and represents an important cause of morbidity and mortality.1–3 Experimental studies have provided evidence about an imbalance between oxidants/antioxidants, in favor of reactive oxidizing species (oxidative stress), associated with COPD.2,4–8 The involvement of oxidative stress in the pathogenesis of COPD appears to be crucial for the manifestation of the inflammatory response of the lung.9–13 The increase of oxidative stress in patients with COPD results from the action of exogenous oxidants (e.g. air pollutants and tobacco components) as well as endogenous oxidants produced during the inflammatory process. However, there are numerous inconsistent results in the studies associated with oxidant and antioxidant imbalance in the pathogenesis of COPD.14,15 One of the main targets of oxidative stress are the polyunsaturated fatty acids present in cell membranes,16,17 the oxidizing species leading to a multistep process in which a whole is classified as lipid peroxidation. There are several products resulting from lipid peroxidation, among those to consider is a dialdehyde (malonyldialdehyde [MDA]) which has a recognized effect on the level of the human genome and is considered a clastogenic and genotoxic agent.18 This means that the evaluation of MDA in biological samples can be considered as an indicator of increased lipid peroxidation and, therefore, an indicator of oxidative damage in vivo.16,19,20
There is evidence that oxidative stress reaches the circulation by a fall in the plasma antioxidant capacity (vitamin C, vitamin E, β-carotene and sulphydryls) associated to smoking. In addition, a similar fall in plasma antioxidant occurs in exacerbations of COPD.5,13 Epidemiological studies have shown that high dietary intake of antioxidants vitamins C and E related to a lower prevalence of chronic bronchitis in smokers.21
The main objective of this study was to clarify the hypothesis of the existence of an imbalance between oxidant species production and antioxidant defence associated with the pathogenesis of COPD.
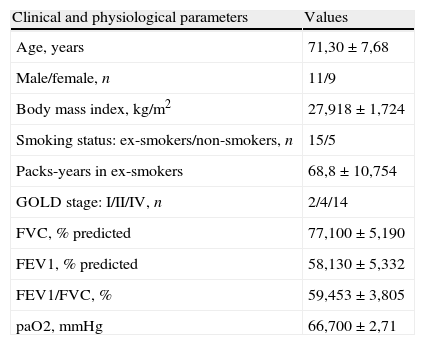
Materials and methodsStudy populationTwenty patients (mean age 71.30±7.68 years) with stable COPD (at least more than 6 months without exacerbation history) were studied. Fifteen of them had a past history of smoking and five were non-smokers, with passive smoking exposure or occupational exposure. Clinical and physiological characteristics of COPD group are shown in Table 1. The ex-smokers had stopped smoking at least 1 year before their participation in the study. Fifty healthy subjects (mean age 41.60±12.31 years; 12 female, 38 male and body mass index, BMI 27.322±4.310kg/m2) with no history of lung disease were used as control group. Twelve of them were current smokers and thirty-eight had never smoked.
Clinical and physiological characteristics of COPD group.
| Clinical and physiological parameters | Values |
| Age, years | 71,30±7,68 |
| Male/female, n | 11/9 |
| Body mass index, kg/m2 | 27,918±1,724 |
| Smoking status: ex-smokers/non-smokers, n | 15/5 |
| Packs-years in ex-smokers | 68,8±10,754 |
| GOLD stage: I/II/IV, n | 2/4/14 |
| FVC, % predicted | 77,100±5,190 |
| FEV1, % predicted | 58,130±5,332 |
| FEV1/FVC, % | 59,453±3,805 |
| paO2, mmHg | 66,700±2,71 |
Oxidative stress was assessed in plasma through the determination of the levels of a biomarker such as MDA in COPD patients and in control group. Antioxidant status was evaluated by the quantification of vitamin C and total sulphydryl (SH) groups, using spectrophotometric methods.
The study was conducted according to the rules of the declaration of Helsinki. Informed consent was obtained from all subjects participating in the study.
MethodsDetermination of plasmatic malonyldialdehydeA biomarker of systemic oxidative stress has been assessed in plasma through the quantification of the levels of a lipid peroxidation derived product, MDA. MDA concentrations were measured spectrophotometrically in terms of thiobarbituric acid reactive substances (TBARS) using a spectrophotometric method modified from Ohkawa et al.22 The absorbances were read at 532nm corresponding to the colored complex formed between the MDA and thiobarbituric acid (TBA). The concentration of TBARS was calculated using the MDA concentration and using a calibration curve previously prepared. The concentration of MDA was expressed in nmol/mL of plasma.
Quantification of vitamin CVitamin C levels were monitored by the method described by Omaye et al.23 In brief, the dinitrophenylhydrazine reacts with oxidized vitamin C (oxidized ascorbic acid) to give a colored product. The absorbance was measured at 520nm and is directly proportional to the vitamin C concentration. The levels of vitamin C were expressed in μg/mL of plasma.
Determination of non-protein sulphydryl groupsThe non-protein sulphydryl groups are mainly in the form of reduced glutathione (GSH). We evaluated the sulphydryl group using a spectrophotometric method involving the use of Ellman's reagent.24 The 5,5′-dithiobis(2-nitrobenzoic acid) (DTNB) undergoes disulfide exchange with sulphydryl groups and 5-thio-2-nitrobenzoate anion (TNB) is formed. The absorbance of the reduced chromogen was measured at 412nm and is directly proportional to the GSH concentration. The levels of sulphydryl groups were expressed in μmol/mL of plasma.
Statistical analysesThe results are expressed as mean±SEM of the concentrations of plasma parameters evaluated. The appropriate nonparametric test was chosen for data not normally distributed. Comparisons between two groups were tested using unpaired t-test or Mann–Whitney U-test. A difference with p<0.05 was considered statistically significant.
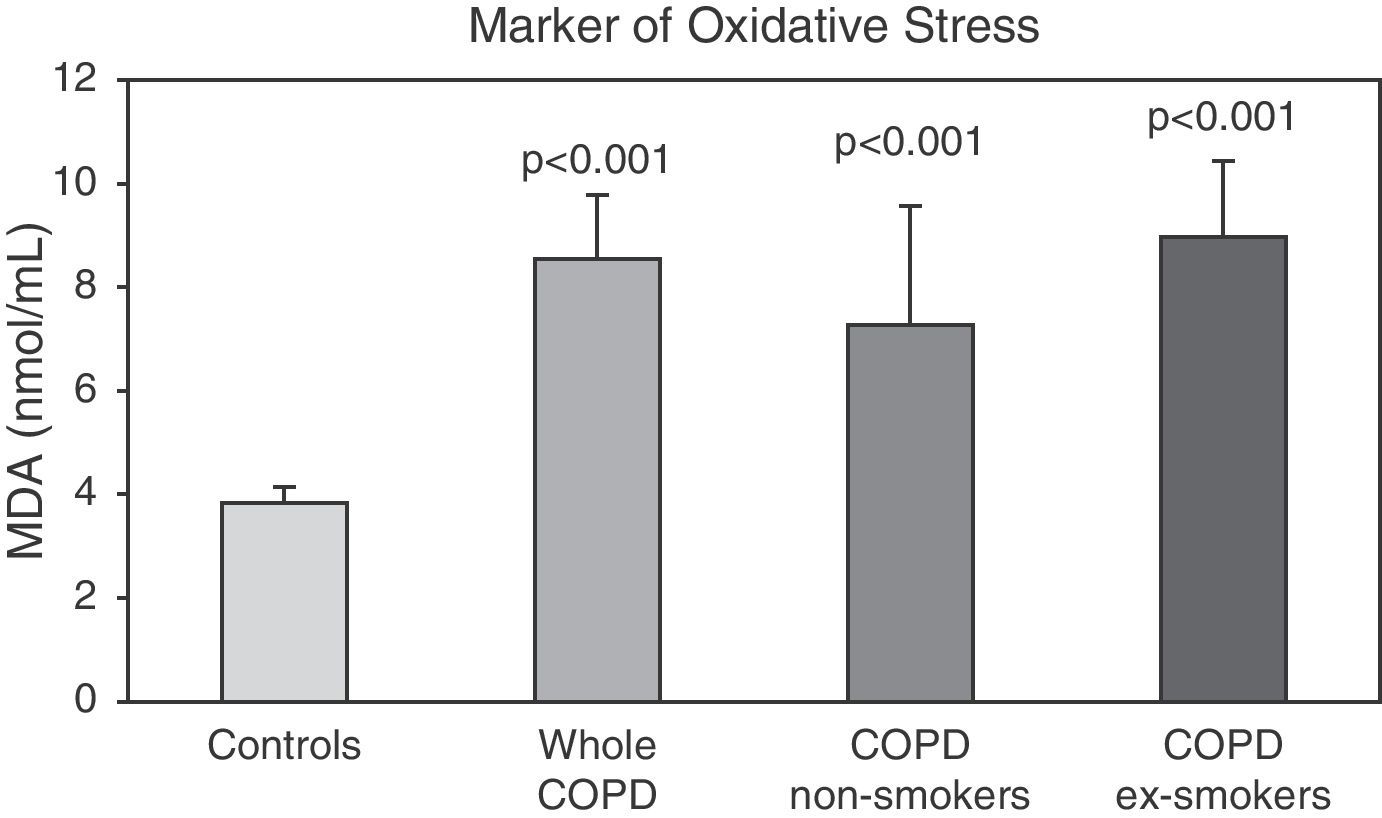
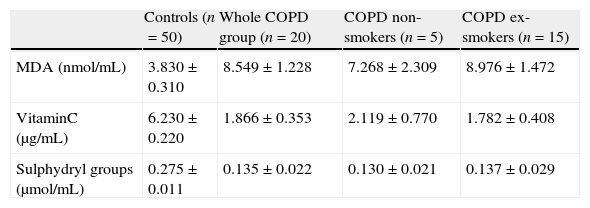
ResultsOxidative stress and antioxidant statusThe plasma concentrations of MDA, vitamin C and sulphydryl groups of COPD patients (whole group, non-smoker and ex-smoker patients) and control subjects are shown in Table 2. The marker of oxidative stress (TBARS evaluated as the amount of MDA produced) was found to be significantly (p<0.001) higher in COPD patients when compared with control group. Fig. 1 shows the MDA plasma levels in controls and COPD patients. We did not find significant differences in MDA levels associated to age but we did observe a significant difference between controls and COPD patients non-smokers (p<0.01) and ex-smokers (p<0.001). Our results have shown no significant difference in TBARS in ex-smokers COPD patients as compared with non-smokers COPD patients. However, we observed an increase in the marker of oxidative stress associated to the ex-smoker patients.
Plasma MDA levels and antioxidant status of the study groups.
| Controls (n=50) | Whole COPD group (n=20) | COPD non-smokers (n=5) | COPD ex-smokers (n=15) | |
| MDA (nmol/mL) | 3.830±0.310 | 8.549±1.228 | 7.268±2.309 | 8.976±1.472 |
| VitaminC (μg/mL) | 6.230±0.220 | 1.866±0.353 | 2.119±0.770 | 1.782±0.408 |
| Sulphydryl groups (μmol/mL) | 0.275±0.011 | 0.135±0.022 | 0.130±0.021 | 0.137±0.029 |
All data are expressed as mean±SEM.
 in plasma from control subjects and COPD patients. Values are expressed as mean±SEM. p<0.001 significantly different between controls and whole COPD group. p<0.01 significantly different between controls and non-smoker patients. p<0.001 significantly different between controls and ex-smoker patients. There was no significant differences between non-smokers and ex-smokers COPD patients.")
Levels of malondialdehyde (MDA) in plasma from control subjects and COPD patients. Values are expressed as mean±SEM. p<0.001 significantly different between controls and whole COPD group. p<0.01 significantly different between controls and non-smoker patients. p<0.001 significantly different between controls and ex-smoker patients. There was no significant differences between non-smokers and ex-smokers COPD patients.
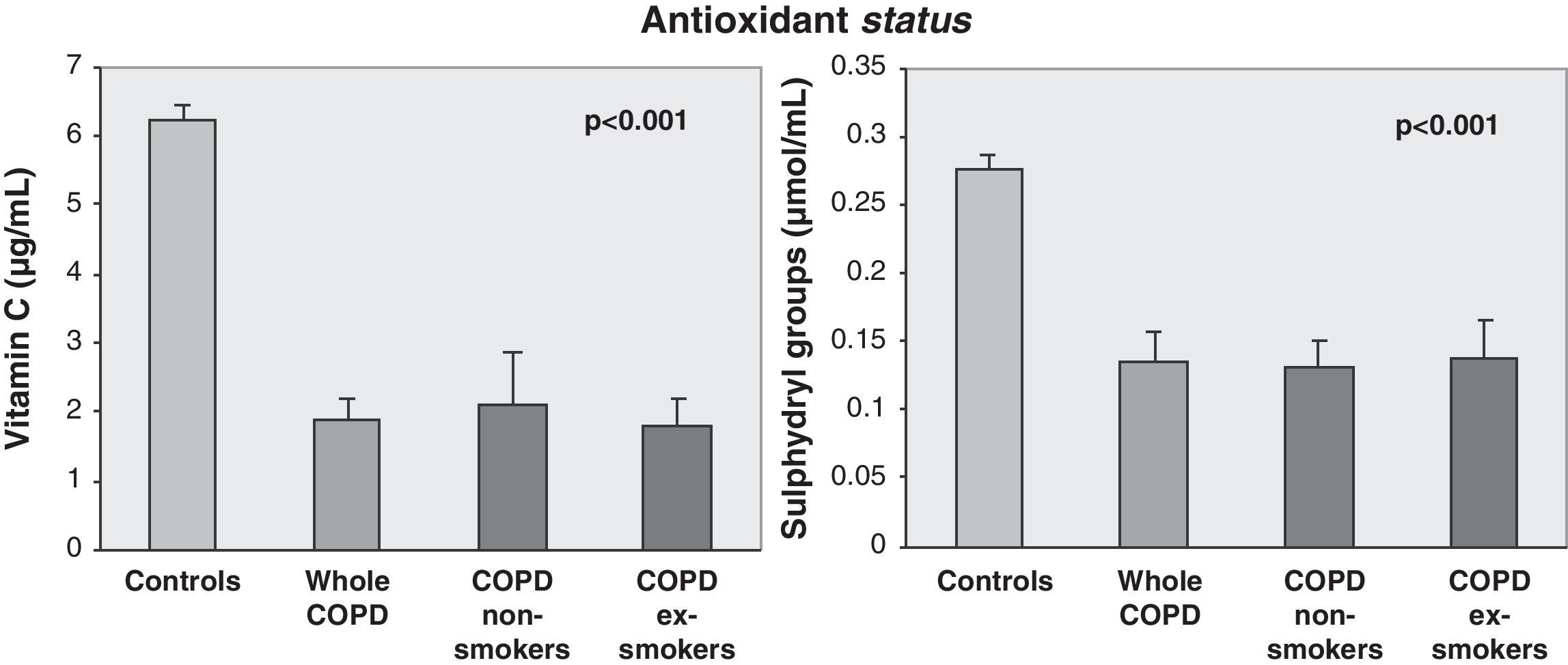
COPD patients had a significant (p<0.001) decrease in antioxidant status (vitamin C and sulphydryl groups) when compared with the control group (Fig. 2). No significant difference was found between non-smokers and ex-smokers in COPD patients. But we observed a decrease in vitamin C associated to the ex-smoker patients.
Discussion and conclusions decrease in antioxidant status (vitamin C and SH groups) when compared with control group.")
Oxidants promote lipid peroxidation in cell membrane. The detection of a product of lipid peroxidation in plasma, namely MDA, is a useful tool to show the occurrence of an oxidative stress in vivo. The aim of the present study was to compare the production of MDA and the levels of antioxidants vitamin C and the thiol groups in COPD and healthy controls. Our results show that oxidative stress is an important pathophysiologic change in COPD. The increase in the lipid peroxidation products in plasma of patients with COPD, supports the hypothesis of oxidative stress associated with the disease. According to our results, an increased oxidative stress is most evident in patients with smoking status, but we did not find significant differences in lipid peroxidation and antioxidant status in non-smokers and ex-smokers patients. In addition, we did not observe any significant difference in the marker of oxidative stress and antioxidant status between healthy smokers and non-smokers. Rahman et al.25 observed that in smokers with and without COPD, an end product of lipid peroxidation is formed in airway epithelial cells, endothelial cells, neutrophils and macrophages. They concluded that oxidative stress resulting from cigarette smoking appears to be more pronounced in those who developed COPD. Previous studies by other authors showed no correlation between TBARs and hydrogen peroxide levels in the COPD associated to cigarette smoking.26 Although our results should be regarded as preliminary, we observed a tendency for an increase in MDA levels associated to COPD patients with smoking habits.
Antioxidants are also markers of oxidative stress. We can define an antioxidant as any substance that, when present at low concentrations, compared with those of the oxidizable substrate, considerably delays or inhibits oxidation of the substrate.16 Antioxidants can act at several different stages in an oxidative sequence. Plasma contains a variety of antioxidants, namely vitamin C and thiol groups. The loss of plasma antioxidants may indicate the ongoing biological oxidative stress. When oxidants increase and antioxidant fail, a situation of oxidative stress ensues that leads to excessive molecular damage and tissue injury.16 Despite some limitations, plasma vitamin C has served as the index for the biochemical evaluation of vitamin C status.23 Plasmatic vitamin C is particularly important because the gas phase of cigarette smoke induces lipid peroxidation in plasma in vitro that is decreased by vitamin C.27 In addition, as a consequence of the role of oxidative stress in the pathogenesis of emphysema, it has been suggested that dietary antioxidants such as vitamins A, C and E could have a protective effect in smokers.3 In addition, other studies showed decreased total antioxidant capacity in patients with COPD as compared to control subjects.28–30 However discrepant results were found in other studies regarding the relationship between antioxidant status and pulmonary functions in COPD patients.14 Other studies failed to find a protective effect of antioxidants on the lung function.30 The molecular mechanisms relating to antioxidant defence in COPD is still lacking.31,32 In this study we found that COPD patients had a significant (p<0.001) decrease in antioxidant status (vitamin C and sulphydryl groups) when compared with control group. The significant decrease in vitamin C and sulphydryl groups associated to COPD patients agrees with the hypothesis that glutathione, the most abundant cellular non-protein sulphydryls, and the glutathione redox cycle may be regarded as an antioxidant mechanism involved in the protection against oxidative stress.33 We did not find a significant difference in the antioxidant status between non-smokers and smokers healthy subjects and between non-smokers and ex-smokers patients but we did observe a tendency toward a decrease in vitamin C associated to COPD patients with smoking habits.
The difference of age between controls and COPD patients could be a limitation in our study. In order to observe the effect of age, we compared the results in healthy subjects younger than 50 years and those over 50 years. We found no significant difference in plasma MDA levels and antioxidant status associated to age. Our observation is supported by the studies of other authors who found no relationship between plasma antioxidant capacity and protein sulphydryls with age in healthy subjects.21,28 Other studies reported no age dependent change in the plasma MDA levels in the general population.34,35 In addition, other authors have found a marked reduction in MDA associated to chronic airway disorders, particularly COPD. It has been suggested that the increase in MDA levels related to the pathophysiology of COPD may be a promising marker of oxidative stress in chronic pulmonary diseases.17
In our study oxygen therapy was not analyzed. However the effect of this therapy in oxidative stress in COPD patients is still controversial. Our results show a significant difference in oxidative stress and antioxidant status between controls and COPD patients (with or without oxygen therapy). No significant difference was found to be associated with oxygen therapy. Further studies are required to clarify the effects of oxygen therapy in COPD patients.
In conclusion, this study showed that elevated levels of TBARS, namely the end product of oxidant stress appears to be more pronounced in COPD patients. Concomitantly, a significant decrease in the protective antioxidant responses was found to be associated to COPD in both non-smokers and ex-smokers patients. The imbalance between oxidants and antioxidants seems to be an important event associated to the development of COPD. This could provide therapeutic implications in the future.
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank Professor J. Mexia who greatly contributed to the Statistical Analyses of this work. We extended our appreciation to patients and the healthy volunteers who generously collaborated in this study.
Please cite this article as: Cristóvão C, et al. Avaliação do equilíbrio entre oxidantes e antioxidantes na patogénese da doença pulmonar obstrutiva crónica. Rev Port Pneumol. 2013. http://dx.doi.org/10.1016/j.rppneu.2012.09.002.
Department where the study was carried out: This study was conducted in the laboratory of Genetics, Faculdade de Medicina, Universidade de Lisboa and in the laboratories of the Universidade Lusófona de Humanidades e Tecnologias de Lisboa.
- Assisted mobilisation in critical patients with COVID-19
- Two years of COVID-19: Trends in rehabilitation
- Comparison of different field tests to assess the physical capacity of post-COVID-19 patients
- New insights in circulating peptidome to differentiate mild to severe COVID-19 patients: Preliminary report
articles


