

To determine patterns of ambulatory oxygen (AO) use among patients with chronic obstructive pulmonary disease (COPD) and interstitial lung diseases, and analyze the effects of this therapy on daily activities and quality of life (QoL).
Patients and methodsWe included 37 consecutive adult patients on AO by liquid O2 for more than three months prescribed by hospital pulmonologists. The acute response to O2 was evaluated through the standardized 6-minutes walk test (6MWT) and the Borg dyspnea scale during the O2 pre-intervention trial. Time spent away from home, compliance, side effects and QoL (SF-36 v1 questionnaire) were evaluated by a telephone interview during the follow-up period. Time spent away from home and QoL comparisons after and before the intervention were assessed retrospectively.
ResultsCOPD was the most frequent diagnosis (54%), and 29 (78%) patients were already on long-term oxygen therapy. In relation to the acute response to O2 evaluated through the 6MWT, there were significant improvements in the distance walked (p<0.001), in resting SatO2 (p<0.001), in minimal SatO2 (p<0.001), and in percentage of desaturation (p=0.002), independently of the diagnosis. No differences were observed in Borg dyspnea scale. AO was used for a mean of 4.1h/day. Patients spent fewer hours per day away from home after AO treatment (3.5h vs. 5.0h, p<0.025). Six patients (16%) were not compliant to the prescription, and 54% mentioned side effects. We verified low scores in almost all of the sub-domains of SF-36 QoL questionnaire, with a significant improvement noted only in emotional role (p=0.032). Improvement in health global state was described by 49% of patients.
ConclusionsAcute improvement in 6MWT parameters was not predictive of enhancement of outdoor activities and QoL with AO. More detailed studies are needed to achieve evidence based AO benefits.
Determinar os padrões de utilização da Oxigenoterapia de Deambulação (OD) em doentes com doença pulmonar obstrutiva crónica (DPOC) e doenças pulmonares intersticiais, e analisar os efeitos dessa terapêutica nas actividades diárias e na qualidade de vida (QV).
Pacientes e métodosForam incluídos consecutivamente 37 doentes adultos sob OD com oxigénio líquido há mais de 3 meses, prescrita por médicos pneumologistas hospitalares. A resposta aguda ao oxigénio foi avaliada através da prova de marcha de 6 minutos (PM6M) e do grau de dispneia de Borg, durante o teste com oxigénio pré-intervenção. O tempo passado fora de casa, a adesão à terapêutica, os efeitos adversos e a QV (questionário SF-36 v1) foram avaliados através de uma entrevista telefónica durante o período de seguimento. A análise comparativa do tempo passado fora de casa e da QV antes e depois da intervenção foi efectuada retrospectivamente.
ResultadosA DPOC foi o diagnóstico mais frequente (54%), e 29 (78%) doentes encontravam-se sob oxigenoterapia de longa duração. Relativamente à resposta aguda ao oxigénio avaliada através da PM6M, houve melhoria significativa na distância percorrida (p<0.001), na SatO2 em repouso (p<0.001), na SatO2 mínima (p<0.001), e na percentagem de dessaturação (p=0.002), independente do diagnóstico. Não foram observadas diferenças no grau de dispneia de Borg. A média de horas de uso da OD foi de 4.1h/dia. Os doentes passaram menos horas por dia fora de casa após tratamento com OD (3.5h vs. 5.0h, p<0.025).
Seis doentes (16%) não cumpriram a terapêutica de acordo com a prescrição, e 54% mencionaram efeitos adversos. Relativamente aos subdomínios do questionário de QV, verificaram-se baixas pontuações em quase todos, com uma melhoria significativa observada apenas no desempenho emocional (p=0.032). Uma melhoria no estado global de saúde foi descrita por 49% dos doentes.
ConclusõesA melhoria aguda constatada nos parâmetros da PM6M não foi preditiva de promoção de actividades no exterior e de melhoria da QV com a OD. São necessários estudos mais detalhados para se constatarem benefícios da OD baseados na evidência.
The benefits of supplemental oxygen use in patients with severe hypoxemia are well established and include increased survival rates,1 decrease in hospitalizations2 improved neuropsychological functions,3 exercise capacity4 and health related quality of life (QoL).5 The benefits were has also been found to be in proportion to the number of hours of daily use3 which justifies the prescription of continuous oxygen therapy. However, the use of oxygen supplementation for such long periods is very demanding, since patients have to be connected to an oxygen supply for all or most of the day, inevitably interfering with their activities, and forcing them to stay at home.
Ambulatory oxygen (AO) consists of oxygen supplementation to patients during exercise and daily activities using a portable device, which means that they are no longer housebound.
Standards of care and guidelines have established criteria for the assessment and prescription of oxygen. In particular, AO therapy prescription is recommended for active patients who are on long-term oxygen therapy (LTOT) for extensive periods and for those that although not eligible for LTOT, desaturate with exercise and show an acute response to oxygen.6,7 In Portugal the existing guidelines (Circular Normativa da Direcção Geral de Saúde N°: 06/DSPCS de 07/06/2006) define the criteria for LTOT prescription- exercise desaturation is one of them, but the specific indications of when to use AO are not explicit. Despite the benefits of oxygen use in enhancing activity8 and improving their QoL, patients have shown low tolerance to its use and are poorly compliant.9 In order to assess the appropriateness of AO therapy, it is important to understand whether patients are in fact using and benefiting from it. The purpose of this study was to determine patterns of AO use among patients with chronic pulmonary disease (COPD) and interstitial lung diseases (ILD) and analyze the effects of this therapy on daily activities and QoL.
Patients and methodsPatientsEligible patients were adults undergoing AO by liquid oxygen for more than 3 months prescribed to use during effort, by hospital pulmonologists in a central hospital of Porto, Portugal. Inclusion criteria consisted of an exercise hypoxemia documented by a standardized 6-minutes walk test (6MWT) on air with evidence of significant desaturation (to 88% or less), responsive to oxygen, and significant daily activity. We considered patients to be significantly active if they were autonomous (not dependent on others for basic daily activities such as getting dressed or taking a bath), not restricted to their homes, except for medical visits, and spending time outside the home for professional or social activities. Patients receiving liquid oxygen for palliative care were excluded.
To better evaluate the AO effects, and based on medical diagnosis and major ventilatory defect identified on lung function tests at baseline, patients were classified in two groups: obstructive ventilatory pattern/ chronic obstructive pulmonary disease (COPD) as defined by the ATS/ERS Statement 200410 (post-bronchodilation FEV1/FVC<70), and restrictive ventilatory pattern/ interstitial lung diseases (ILD) (normal or increased FEV1/FVC ratio and total lung capacity<80% of predicted). The ILD group included patients with hypersensitivity pneumonitis, silicosis, sarcoidosis, idiopathic pulmonary fibrosis and connective tissues diseases related pulmonary disease.
Study designPatient baseline data were collected retrospectively through medical files consultation and, they included demographic data, pre-treatment spirometry, lung volumes, CO diffusion capacity (Masterscreen Body Diffusion – Vmax 62, Viasys Healthcare), resting arterial blood gases on air (RapidLab 1265 – Siemens) and the results of the 6MWT performed on air and on oxygen.
Acute efficacy of AO was assessed objectively in all patients before the intervention by a 6MWT with and without oxygen to support AO prescription.
Oxygen saturation (SatO2) was monitored through finger pulse oximeter (Pulsox-3i, Konica Minolta) at rest and during the 6MWT. Patients repeated 6MWT receiving supplemental oxygen by a liquid-oxygen stroller in increments of 1L/min to the point of the lowest oxygen flow rate to maintain the SatO2 saturation ≥90%. Evaluation of dyspnea was estimated by the modified Borg scale (0 – 10)11 at rest and at the end of the exercise.
Patients were interviewed by telephone by a physician during the month of July 2009. Information collected concerned medical history, professional situation, smoking habits, number of hours and circumstances of AO prescription, compliance (AO use during outings or during effort), patterns of oxygen use (data presented on Table 3) and side effects. A questionnaire to assess QoL (the short form (SF)-36 version 1) was also conducted by telephone.
While efficacy of AO was assessed objectively in the acute setting, patterns of AO use and long-term AO efficacy were evaluated in a subjective fashion through a questionnaire during the interview. To assess QoL after the intervention, patients were asked to evaluate their QoL taking into consideration their most recent period of stabilization, and then, report back to the time before they started using it to evaluate QoL before the intervention. The SF-36 v1 QoL questionnaire was chosen on the basis that it is the most extensively validated and commonly used health survey instrument for appraising QoL.12 It has two components (physical, mental) and eight sub-domain scores (physical functioning, physical role, bodily pain, general health, vitality, social functioning, emotional role, mental health). A supplementary question was asked regarding their global health state compared with AO pre-treatment.
The study received approval from the local research committee (Unidade Integrada de Gestão de processos documentais).
Statistical methodsFor each variable, we used standard methods to calculate proportions, means and standard deviations (SD). Between-group comparisons of the patients’ baseline characteristics as well as compliance were made with unpaired t-test or Chi-square test when appropriate. Comparisons of parameters before and after the AO prescription were analyzed by an ANOVA general linear model for repeated measures. Besides the whole group comparison of the two conditions (air vs. O2) (within-subjects effect), between-groups differences were explored (between-subjects effect) and also whether the AO effects were dependent on the diagnosis group (interaction). The results were considered statistically significant when p-values were <0.05. The data were analyzed using the SPSS-17 statistical program.
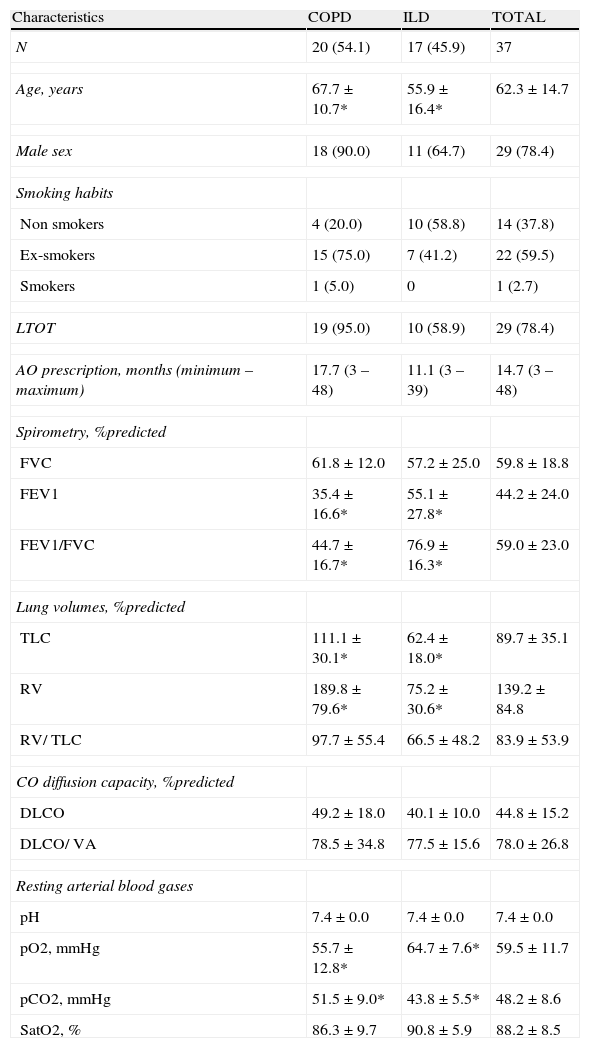
ResultsPatients’ baseline characteristicsFrom a total of 45 patients meeting the inclusion criteria, 3 had moved out of the residence area waiting for transplant abroad and 5 were inaccessible. Thirty-seven patients completed the study by telephone interview. Their baseline characteristics are shown in Table 1. COPD patients were older (p=0.013), more severely hypoxemic (p=0.025), and more hypercapnic (p=0.008).
Baseline characteristics of the study patients.
| Characteristics | COPD | ILD | TOTAL |
| N | 20 (54.1) | 17 (45.9) | 37 |
| Age, years | 67.7±10.7* | 55.9±16.4* | 62.3±14.7 |
| Male sex | 18 (90.0) | 11 (64.7) | 29 (78.4) |
| Smoking habits | |||
| Non smokers | 4 (20.0) | 10 (58.8) | 14 (37.8) |
| Ex-smokers | 15 (75.0) | 7 (41.2) | 22 (59.5) |
| Smokers | 1 (5.0) | 0 | 1 (2.7) |
| LTOT | 19 (95.0) | 10 (58.9) | 29 (78.4) |
| AO prescription, months (minimum – maximum) | 17.7 (3 – 48) | 11.1 (3 – 39) | 14.7 (3 – 48) |
| Spirometry, %predicted | |||
| FVC | 61.8±12.0 | 57.2±25.0 | 59.8±18.8 |
| FEV1 | 35.4±16.6* | 55.1±27.8* | 44.2±24.0 |
| FEV1/FVC | 44.7±16.7* | 76.9±16.3* | 59.0±23.0 |
| Lung volumes, %predicted | |||
| TLC | 111.1±30.1* | 62.4±18.0* | 89.7±35.1 |
| RV | 189.8±79.6* | 75.2±30.6* | 139.2±84.8 |
| RV/ TLC | 97.7±55.4 | 66.5±48.2 | 83.9±53.9 |
| CO diffusion capacity, %predicted | |||
| DLCO | 49.2±18.0 | 40.1±10.0 | 44.8±15.2 |
| DLCO/ VA | 78.5±34.8 | 77.5±15.6 | 78.0±26.8 |
| Resting arterial blood gases | |||
| pH | 7.4±0.0 | 7.4±0.0 | 7.4±0.0 |
| pO2, mmHg | 55.7±12.8* | 64.7±7.6* | 59.5±11.7 |
| pCO2, mmHg | 51.5±9.0* | 43.8±5.5* | 48.2±8.6 |
| SatO2, % | 86.3±9.7 | 90.8±5.9 | 88.2±8.5 |
Data are presented as mean±standard deviation (SD) or No. (%) unless otherwise indicated; * - Statistical significant differences between groups; COPD – chronic obstructive pulmonary disease; ILD – interstitial lung diseases; LTOT – long-term oxygen therapy; AO – ambulatory oxygen; FVC – forced vital capacity; FEV1 – forced expiratory volume in first second; TLC – total lung capacity; RV – residual volume; DLCO – diffusing capacity of lung for carbon monoxide; VA – alveolar volume; pO2 – oxygen arterial pressure; pCO2 – carbon dioxide arterial pressure; SatO2 – arterial saturation.
With respect to patients’ diagnosis, COPD was the most frequent (54.1%) representing the strongest reason for AO prescription. Heart failure, other cardiovascular abnormalities or respiratory muscle weakness were not found as primary reasons for prescribing AO. Pulmonary tuberculosis sequelae and bronchiectasis were not isolated criteria for prescription, but constituted secondary diagnosis in 18.9% and 13.5% of cases, respectively. A subset of patients also had obstructive sleep apnea syndrome as a co-morbid condition (13.5%), requiring, in addition to AO, a nightly regimen of positive-airway-pressure therapy.
Of the study participants, 14 (37.8%) were non smokers, 22 (59.5%) were ex-smokers and 1 (2.7%) maintained smoking habits. Concerning professional situation, 30 (81.1%) were retired, 6 (16.2%) on sick-leave and 1 (2.7%) unemployed. The majority of patients lived with other people (family or caregivers) in 89.2% of cases.
Of the 37 patients, 29 (78.4%) were on LTOT, predominantly those in the COPD group (95.0% vs. 58.8%, p=0.008). Five (13.5%) patients were in rehabilitation programs at the time of the telephone interview and 3 (8.1%) had a history of emergency visits or hospitalizations in the 2 months prior the telephone interview.
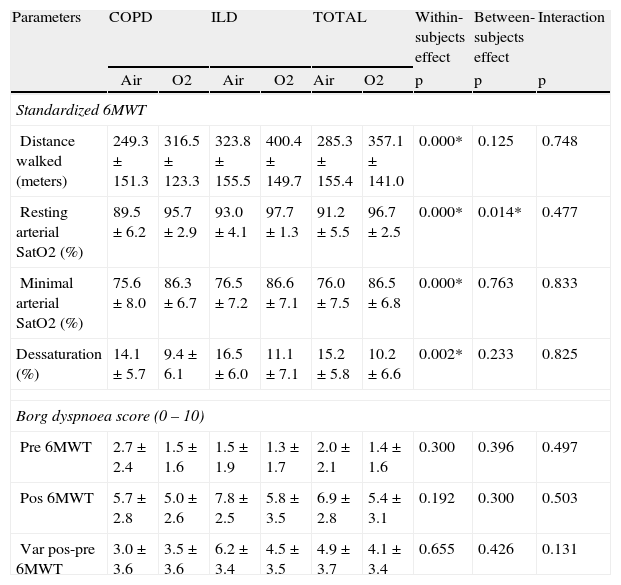
Acute response to oxygen - 6MWT objective parametersConcerning the 6MWT on air compared with oxygen, there were significant improvements in the distance walked (285.3m vs. 357.1m, p<0.001), in resting SatO2 (91% vs. 98%, p<0.001), in minimal SatO2 (76.0% vs. 86.5%, p<0.001), and in percentage of desaturation (15.2% vs. 10.2%, p=0.002). These improvements were independent of the diagnosis (Table 2). No statistical differences were noted between COPD and ILD groups for all parameters of standardized 6MWT.
Oxygen response in standardized 6-minutes walk test.
| Parameters | COPD | ILD | TOTAL | Within-subjects effect | Between-subjects effect | Interaction | |||
| Air | O2 | Air | O2 | Air | O2 | p | p | p | |
| Standardized 6MWT | |||||||||
| Distance walked (meters) | 249.3±151.3 | 316.5±123.3 | 323.8±155.5 | 400.4±149.7 | 285.3±155.4 | 357.1±141.0 | 0.000* | 0.125 | 0.748 |
| Resting arterial SatO2 (%) | 89.5±6.2 | 95.7±2.9 | 93.0±4.1 | 97.7±1.3 | 91.2±5.5 | 96.7±2.5 | 0.000* | 0.014* | 0.477 |
| Minimal arterial SatO2 (%) | 75.6±8.0 | 86.3±6.7 | 76.5±7.2 | 86.6±7.1 | 76.0±7.5 | 86.5±6.8 | 0.000* | 0.763 | 0.833 |
| Dessaturation (%) | 14.1±5.7 | 9.4±6.1 | 16.5±6.0 | 11.1±7.1 | 15.2±5.8 | 10.2±6.6 | 0.002* | 0.233 | 0.825 |
| Borg dyspnoea score (0 – 10) | |||||||||
| Pre 6MWT | 2.7±2.4 | 1.5±1.6 | 1.5±1.9 | 1.3±1.7 | 2.0±2.1 | 1.4±1.6 | 0.300 | 0.396 | 0.497 |
| Pos 6MWT | 5.7±2.8 | 5.0±2.6 | 7.8±2.5 | 5.8±3.5 | 6.9±2.8 | 5.4±3.1 | 0.192 | 0.300 | 0.503 |
| Var pos-pre 6MWT | 3.0±3.6 | 3.5±3.6 | 6.2±3.4 | 4.5±3.5 | 4.9±3.7 | 4.1±3.4 | 0.655 | 0.426 | 0.131 |
6MWT - 6-minutes walk test; COPD – chronic obstructive pulmonary disease; ILD – interstitial lung diseases; SatO2 – arterial saturation in oxygen; var – variation, * – statistical significant values.
Borg dyspnea scale data were available in only 14 of the 37 patients.
On the basis of the pre and post-6MWT Borg dyspnea scale with air compared with oxygen, no differences were observed within subjects, between subjects or for the effects of interaction. Additionally we performed an analysis of the 6MWT Borg dyspnea scale variation (post - pre), which showed no significant differences (Table 2). The patients who decreased at least 1 point in Borg dyspnea scale on oxygen were not predominantly from any of the defined groups, either on pre-6MWT (p=0.310) or on post-6MWT (p=0.533).
Patterns of AO usage and complianceMedical prescription varied regarding the number of hours the patient should use AO, but all patients were instructed to use it in effort and in every outing.
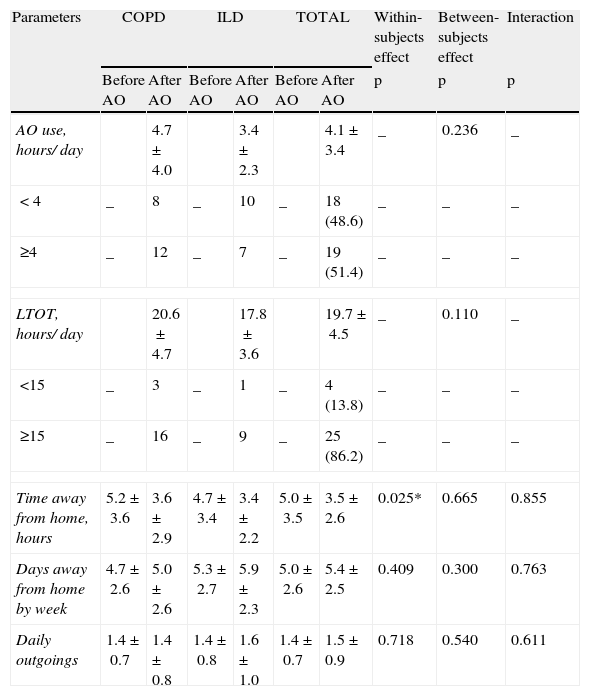
When asked the question “how many hours a day do you use liquid oxygen through the portable device?” patients said they used it for a mean of 4.1h/day (Table 3). No differences were found between COPD and ILD groups (4.7±4.0h vs. 3.4±2.3h, p=0.236), or between patients on LTOT compared with AO alone (4.4±3.6h vs 3.0±2.1h, p=0.301). The number of hours of AO use was not significantly higher in patients that improved in Borg dyspnea score in the acute response to oxygen (4.2±1.9h vs. 3.7±3.5h, p=0.787).
Oxygen use and time spent away from home.
| Parameters | COPD | ILD | TOTAL | Within-subjects effect | Between-subjects effect | Interaction | |||
| Before AO | After AO | Before AO | After AO | Before AO | After AO | p | p | p | |
| AO use, hours/ day | 4.7±4.0 | 3.4±2.3 | 4.1±3.4 | _ | 0.236 | _ | |||
| < 4 | _ | 8 | _ | 10 | _ | 18 (48.6) | _ | _ | _ |
| ≥4 | _ | 12 | _ | 7 | _ | 19 (51.4) | _ | _ | _ |
| LTOT, hours/ day | 20.6±4.7 | 17.8±3.6 | 19.7±4.5 | _ | 0.110 | _ | |||
| <15 | _ | 3 | _ | 1 | _ | 4 (13.8) | _ | _ | _ |
| ≥15 | _ | 16 | _ | 9 | _ | 25 (86.2) | _ | _ | _ |
| Time away from home, hours | 5.2±3.6 | 3.6±2.9 | 4.7±3.4 | 3.4±2.2 | 5.0±3.5 | 3.5±2.6 | 0.025* | 0.665 | 0.855 |
| Days away from home by week | 4.7±2.6 | 5.0±2.6 | 5.3±2.7 | 5.9±2.3 | 5.0±2.6 | 5.4±2.5 | 0.409 | 0.300 | 0.763 |
| Daily outgoings | 1.4±0.7 | 1.4±0.8 | 1.4±0.8 | 1.6±1.0 | 1.4±0.7 | 1.5±0.9 | 0.718 | 0.540 | 0.611 |
Data are presented as mean±standard deviation (SD) or No. (%); AO – ambulatory oxygen; COPD – chronic obstructive pulmonary disease; ILD – interstitial lung diseases; * – statistical significant value.
With regard to time spent in outdoor activities, patients spent fewer hours per day away from home after AO treatment (3.5±2.6h vs. 5.0±3.5h, p<0.025) (Table 3). This fact was not influenced by the improvement or otherwise in Borg dyspnea score. No significant differences were recorded in the days away from home per week and in daily outings.
Six patients (16.2%) were not compliant to the prescription, using AO for 0.9±0.5h/ day. Additionally, 54.1% mentioned side effects, like nasal discomfort, the device being too heavy or embarrassment. Compliance was independent of the diagnosis, of whether patients used LTOT or not (89.7% and 62.5% of patients respectively, were compliant, p=0.065) and was not related to patient age (61.7±14.1 years old vs. 65.3±18.3 years old, p=0.583, for compliant and non compliant patients respectively).
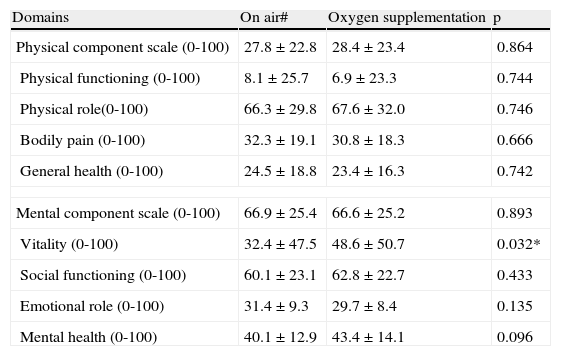
Quality of life evaluationAfter treatment we verified low scores in almost all sub-domains of SF-36 QoL questionnaire, mainly in physical role (6.9%), vitality (23.4%), physical functioning (28.4%) and general health (30.8%), with the best performances in mental health (62.8%), bodily pain (67.6%) and social functioning (66.6%). A significant improvement was only noted in emotional role (32.4% vs. 48.6%, p=0.032) (Table 4). An improvement in global health state compared with pre-treatment was stated by 46% of patients in opposite to 35% who described worsening.
Assessment of quality of life by SF-36 questionnaire.
| Domains | On air# | Oxygen supplementation | p |
| Physical component scale (0-100) | 27.8±22.8 | 28.4±23.4 | 0.864 |
| Physical functioning (0-100) | 8.1±25.7 | 6.9±23.3 | 0.744 |
| Physical role(0-100) | 66.3±29.8 | 67.6±32.0 | 0.746 |
| Bodily pain (0-100) | 32.3±19.1 | 30.8±18.3 | 0.666 |
| General health (0-100) | 24.5±18.8 | 23.4±16.3 | 0.742 |
| Mental component scale (0-100) | 66.9±25.4 | 66.6±25.2 | 0.893 |
| Vitality (0-100) | 32.4±47.5 | 48.6±50.7 | 0.032* |
| Social functioning (0-100) | 60.1±23.1 | 62.8±22.7 | 0.433 |
| Emotional role (0-100) | 31.4±9.3 | 29.7±8.4 | 0.135 |
| Mental health (0-100) | 40.1±12.9 | 43.4±14.1 | 0.096 |
Data are presented as %±standard deviation; # – retrospective responses compared with oxygen supplementation; * – statistical significant value.
The aim of this study was to assess the efficacy and patterns of AO usage by liquid oxygen in patients with chronic respiratory diseases independently of LTOT therapy prescription. LTOT benefits have been proven mainly in studies of COPD patients,1,3 with the results being extrapolated to hypoxemic patients with other diagnosis.13 Consequently oxygen therapy became routine treatment for all severely hypoxemic patients. The same applied to patients not fulfilling LTOT criteria but desaturating with exercise, when it comes to AO. One study found out that improvement in exercise ability and reduction in breathlessness with AO could be achieved both in COPD and ILD patients.14 Our patients therefore included several diagnoses which were grouped according to their ventilatory pattern.
Although exercise capacity is a good prognosis factor for survival in COPD patients,15 we cannot expect survival benefits of AO in the context of current knowledge because studies assessing long-term benefits of AO do not allow us to draw any firm conclusions concerning the effectiveness of AO.16
When LTOT is prescribed, it is intended to be used for long periods and is traditionally provided by 2 types of large stationary systems: a gaseous-oxygen cylinder or an oxygen concentrator. To facilitate movement in and about the home, patients can be connected to their stationary system by up to 15 meters of supply tubing.17 But to ambulate beyond that distance, either within the home or out into the community, a portable oxygen device will be required. The major goals of AO are thus to enable the patients to leave their homes for a longer period of time, to improve health status, and to increase daily activities.
AO can also be provided by 2 ways: small gaseous-oxygen cylinders that can be pulled on a cart, but have limited oxygen capacity18; or a liquid oxygen system, which was used by our patients. The latter consists of a main base unit container (referred to as a “dewar”) that stores oxygen in its liquid state at -170°C and a small portable oxygen-delivery system, that the patient can refill from the stationary dewar prior to ambulation. This portable option has several advantages, it is small in size and has a larger capacity, and therefore more cost-effective for patients with high daily activity.18 If patients are also on LTOT, they can use the stationary dewar in the same way as the gaseous oxygen container or concentrator to receive oxygen during rest. In this way, liquid oxygen can became the only source of supplemental oxygen, used for both purposes.
Our results showed that patients had a positive acute response to oxygen, assessed by the 6MWT, validating OA prescriptions.7 Nevertheless, the subjective sensation of dyspnea assessed by Borg scale, did not improve, at least during the in-laboratory test. Previous studies are contradictory with regard to the benefits of acute oxygen supply for exercise tolerance and the associated dyspnea. A systematic review of 31 randomized controlled trials demonstrated that AO was effective in increasing exercise capacity and reducing breathlessness in patients with exercise desaturation.19 More recently, Héraud et al concluded that oxygen supply does not systematically improve exercise tolerance in all patients. In about one third a negative response with a paradoxical increase in breathing frequency and dyspnea was observed.20
Concerning the long-term benefits in QoL and time spent in outdoor activities our results do not clearly support the prescription of AO. No improvements were noticed in QoL score values, except for emotional role (32.4% vs. 48.6%, p=0.032), and patients spent fewer hours per day outdoors at the time of the study than before AO treatment. Reported side-effects like embarrassment and device weight could account for some of the inhibition to get outside, but the disease aggravation (a proportion of 35% patients described worsening of global health state) could also be responsible. The failure of AO to increase activity or improve QoL has been previously reported9,21–23. A recent randomized trial of domiciliary AO (cylinder air versus cylinder oxygen) in patients with COPD and dyspnea but without hypoxemia also showed no benefits for either groups in terms of dyspnea, QoL, functional status or cylinder utilization. Statistically significant but clinically small improvements in dyspnea and depression were observed in the study group as a whole over the 12 weeks of the study, probably representing a placebo benefit.24 In contrast, Eaton et al, in a study of 41 COPD patients with exercise desaturation reported a statistically significant, albeit clinically small, improvement in QoL, anxiety and depression.25,26
There are some positive aspects related to QoL. In spite of the complex interplay of functional and psychosocial disability that affects these patients, emotional role was improved, and 46.0% referred to a subjective improvement in their health global state. Patient perspectives about the use of AO should be taken into account and it is interesting that 4 patients said that they would never leave their home without oxygen, although this point was not included in the questionnaire. Their experience may be attributed to a learned oxygen-related decrease in exertional dyspnea in daily activities, despite dyspnea relief was not sensed in 6MWT.9 As suggested by other studies, a placebo effect cannot be excluded.27
The number of hours of AO useper day (4.1h) was similar to the hours spent outside the home (3.5h), and was quite high. It is remarkable that patients left the house almost every day, despite their respiratory morbidity. Other studies have reported a lack of use of AO,28 or its inappropriate use at rest,29 which did not seem to occur with our patients. The non-compliance rate was low and all of the compliant patients, with 3 exceptions, used AO more than 1h/day, which can be accepted as a reasonable use.30
Pépin J et al reported a more effective oxygen use with the duration of the treatment29, which the authors suggested could be due to the deterioration in respiratory function over time but could also be related to the effects of technical and medical education of the patient. Vergeret et al29 have also shown the association between good compliance and the severity of the patient's condition. We consider that our patients did in fact have a high level of compliance (83.8%), for various reasons, including severity of the disease (78.4% were on LTOT), more effective use with time (mean time of AO prescription of 14.7 months) and more repeated education from health-care professionals. However, since compliance was assessed in a subjective fashion, there is the possibility that patient may have overestimated their use of AO.28,29
No significant differences appear to exist in the efficacy of AO (hours of use and compliance) between patients on LTOT compared with AO alone. In other studies AO prescription seemed to lead to a more effective use of LTOT29 and increased compliance,28 but the number of patients in our study does not allow us to take firm conclusions on this.
One limitation of our work was that some Borg scale data were not available, which has conditioned the identification of significant responses to AO. Taking into account previous studies reporting conflicting results about dyspnea relief29 we hypothesized that patients with the best improvements in Borg dyspnea scale could be more prone to use and benefit from AO, but this could not be proved in our study. Used oxygen flow rates were not evaluated, which could also have interfered with the response to AO, since low flow rates may provide inadequate relief of exercise dyspnea.23 The type of protocol used to assess the exercise performance can explain some of the variability in reported benefits of supplemental oxygen.8 Davidson et al reported that the endurance walking test was equally sensitive as a more formal assessment on a cycle ergometer and more reliable than the commonly used 6MWT. All these insights must be considered in future studies.
Time spent away from home and QoL baseline evaluation were collected retrospectively, with some patients having to remember things from up to 4 years earlier, which may have led to recall bias. A prospective study may overcome such limitations and in addition may explore the effect of time and education on AO use.
As far as we know, this is the first study in our country to evaluate the use and efficacy of AO. Since AO therapy does have its side-effects and costs, this information is of prime importance to patients, clinicians and health-care policy programs, as is the ability to distinguish patients who would benefit from this treatment. We observed that the acute improvement in 6MWT parameters did not help to predict the long-term benefits related to the enhancement of outdoor activities and QoL, as we would have expected. Desaturation in 6MWT also does not seem to be a reliable criterion for selecting the patients who should be prescribed AO. As well as acute response to oxygen, other factors like improved Borg dyspnea scale, the severity of disease, patient motivation or education, could influence the use and benefits of AO. In this way, a detailed assessment of individual patient response with a standardized follow-up with more frequent medical and technical monitoring, might achieve evidence based AO benefits. Our results point to the need of broader and more detailed studies evaluating these parameters and including more accurate assessment of patients’ activities, AO use and efficacy.
Conflicts of interestThe authors have no conflicts of interest to declare.
Please cite this article as: Vieira T, et al. Eficácia e padrões de utilização da oxigenoterapia de deambulação de um hospital universitário. Rev Port Pneumol. 2011; 17: 159–167.


