

A comprehensive knowledge of the normal pattern of endobronchial branching is essential to any pulmonologist. The classification systems available are predominantly static descriptions and only seldom do they refer to possible variations within the normal spectrum.
To evaluate all possible anatomical variants of the tracheobronchial tree we conducted a prospective study in our endoscopy unit between February 1st and July 10th 2009.
A total of 181 individuals were included in the study. Anatomical variants were found to be present in 79 individuals (43% of total). Overall we found 20 different anatomical variants. Variations were more frequently found within the right upper lobe (16.6% of individuals). Middle lobe and lingula presented no variations. The variant most frequently found was the presence of a bifurcate pattern of the right upper bronchus (13.8%).
The present study revealed a relatively high frequency of anatomical alternatives to the normal endobronchial branching pattern. Recognition of these variants and the frequency of their expression are fundamental for the bronchologist in establishing the limits of normal anatomy and preparing endobronchial techniques or surgical procedures.
O conhecimento detalhado do normal padrão de ramificações da árvore traqueobrônquica é um requisito essencial para qualquer pneumologista. Os sistemas de classificação funcional que guiam a prática clínica corrente têm um carácter eminentemente estático e raramente contemplam referências aos desvios possíveis dentro do espectro normal.
Por forma a caracterizar as variações anatómicas da árvore traqueobrônquica, os autores desenvolveram um estudo prospectivo que decorreu entre Fevereiro e Julho de 2009, onde se incluíram todos os doentes referenciados para realização de broncofibroscopias diagnósticas e/ou terapêuticas.
Um total de 181 indivíduos foram incluídos no estudo tendo-se observado variantes anatómicas em 79 (43% do total). Globalmente observamos 20 diferentes variantes anatómicas. Estas variantes foram mais frequentemente observadas no lobo superior direito (16,6%). O lobo médio e a língula não foram sede de variantes anatómicas. A variante mais frequentemente observada foi o padrão bifurcado do lobo superior direito (13,8%).
O presente estudo revelou uma elevada frequência de formas alternativas ao clássico padrão de ramificação traqueobrônquica. O conhecimento da tipologia, morfologia e frequência de expressão dessas variantes revela-se de extrema importância para o broncologista no estabelecimento das fronteiras da anatomia normal e na planificação de técnicas endoscópicas ou de procedimentos cirúrgicos.
One can say that ever since the first endobronchial observations were carried out by Killian with the rigid bronchoscope, the characterization of the tracheobronchial anatomy has been the subject of great debate.
Jakson and Huber1 were the first ones to recognize the importance of a systematic classification of the tracheobronchial tree. In fact their classification system presented in 1943 would end up as the basis of the international nomenclature system approved by the British Thoracic Society in 1949.2
The subsequent development of fiberoptic bronchoscopy by Ikeda led to further characterizations of the endobronchial anatomy, due mainly to the contributions of Ikeda himself3 and Nagaishi.4
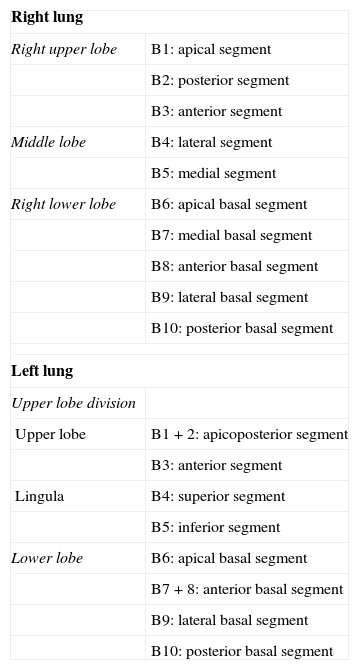
This would ultimately lead to successive revisions of the international classification system such as the one presented by Collins in 19875 which still use today (Table 1).
Revision of the international nomenclature of the endobronchial tree (Collins et al.5).
| Right lung | |
| Right upper lobe | B1: apical segment |
| B2: posterior segment | |
| B3: anterior segment | |
| Middle lobe | B4: lateral segment |
| B5: medial segment | |
| Right lower lobe | B6: apical basal segment |
| B7: medial basal segment | |
| B8: anterior basal segment | |
| B9: lateral basal segment | |
| B10: posterior basal segment | |
| Left lung | |
| Upper lobe division | |
| Upper lobe | B1+2: apicoposterior segment |
| B3: anterior segment | |
| Lingula | B4: superior segment |
| B5: inferior segment | |
| Lower lobe | B6: apical basal segment |
| B7+8: anterior basal segment | |
| B9: lateral basal segment | |
| B10: posterior basal segment | |
But despite their undeniable utility, all of the systems of classification presented over the years have been predominantly static descriptions and only seldom do they refer to possible variations within the normal spectrum.
These variations are believed to be the result of embryonic disturbances of the normal branching pattern,6 but the aetiology of this phenomenon has never really been understood.
Besides Prakash7 who only mentions the possibility of normal variations, without referring to the frequency of occurrence, there are few studies that address this issue. Gonlugur et al.8 described the presence of variations of the branching pattern in 2.6% of a total of 2550 exams analysed retrospectively. Right upper lobe bifurcation pattern was the most frequent variation found. The variations were predominantly found in male patients. A single prospective study conducted within the Turkish population retrieved parallel results with further characterization of other different but rarer variations.9
ObjectivesTo evaluate all possible anatomical variants of the tracheobronchial tree which were present in adult individuals who underwent fiberoptic bronchoscopy in our unit.
Material and methodsWe conducted a prospective study, which was carried out in our unit between February 1st and July 10th 2009 and which included a total of 181 individuals who had undergone fiberoptic bronchoscopy for either diagnostic or therapeutic purposes.
We systematically reviewed the endobronchial anatomy and registered both graphic (photograph or video whenever possible) and descriptive (exam report and specific database) information regarding anatomical variants observed (with reference to the classification presented by Collins et al. –Table 1).
We used SPSS 17.0 software (SPSS Inc., Chicago, IL, USA) to perform all statistical analysis of clinical data. Associations among the different variables were performed using the Pearson's chi-square test. Results were considered statistically significant for p values under 5%.
ResultsDuring the period of this study a total of 221 exams (in 207 patients) were performed in our unit. Of this total, 26 patients were excluded: 9 because the exams were performed by physicians not participating in the study; 9 because the exam only allowed inspection of the trachea (4 during the course of fiberoptic guided oro/naso-tracheal intubation and 5 because of tracheal stenosis); and 8 because of gross anatomical alterations due to tumour invasion, surgical resections or previous pulmonary tuberculosis.
All individuals included were Caucasian adults with an average age of 63 years (minimum: 23; maximum: 95) and male predominance (66%).
Anatomical variants were found to be present in 79 individuals (43% of total). These subjects had an average age of 63 years and were predominantly male (62%).
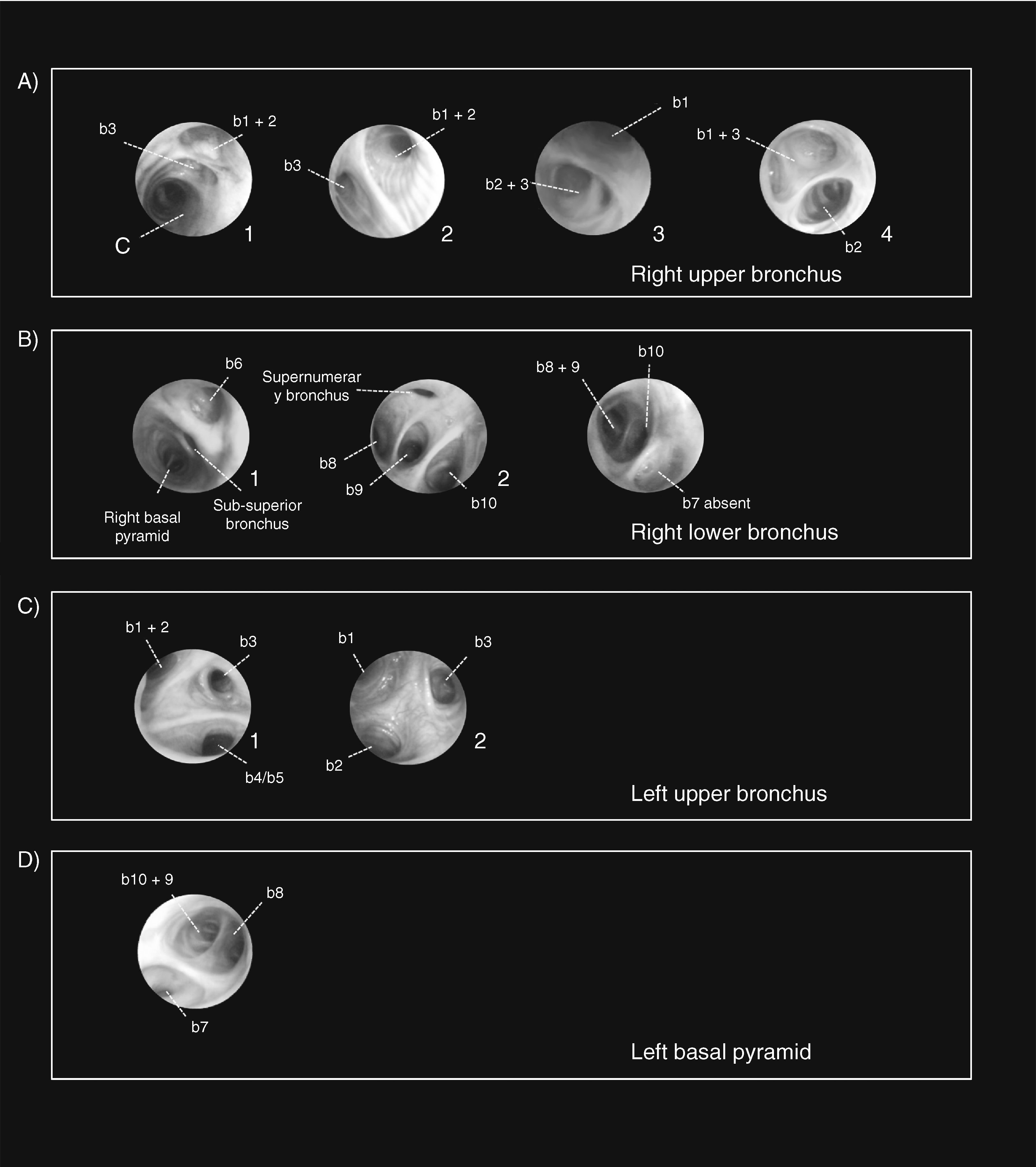
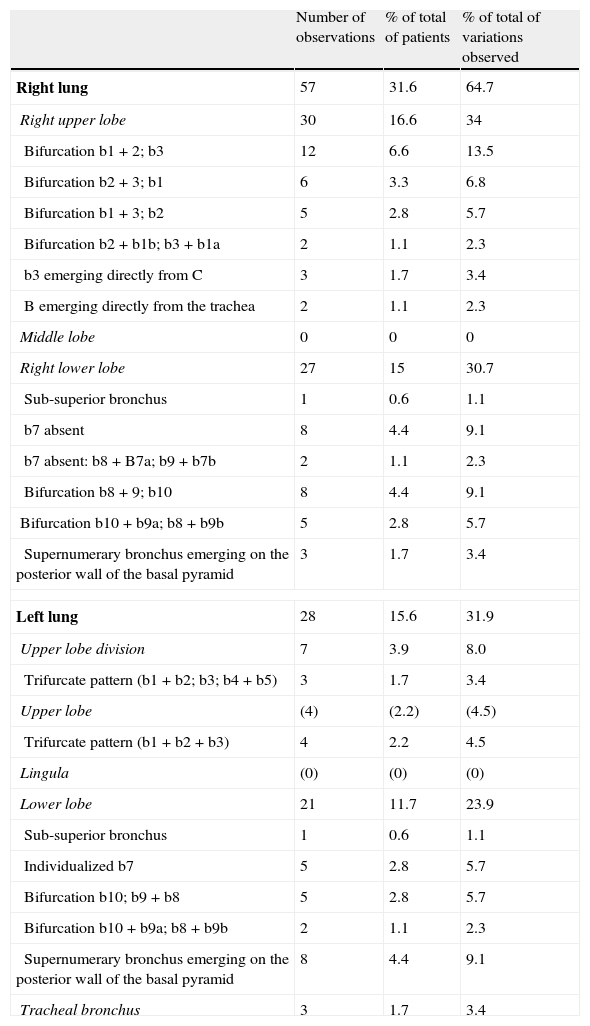
Overall we found 20 different anatomical variants (Table 2). Variations were most frequently found within the right upper lobe (16.6% of individuals). In this location, four different patterns of bifurcation and two other anatomical variants could be observed (Table 2 and Fig. 1A1–A4). A rarer anatomical alternative that we observed in two patients was a right upper bronchus emerging directly from the lower tracheal wall, above the main carina. The left upper lobe, on the other hand, presented only two anatomical alternatives to the normal branching pattern. The first one was a trifurcate pattern of the upper lobe division, meaning that b1+b2; b3; b4+b5 emerged independently but all at the same level, as opposed to the more common bifurcation of the upper lobe division (giving rise to the upper bronchus – subsequently divided into b1+b2; b3) and the lingular bronchus (further divided into b4+b5). The second was the presence of a trifurcate pattern of the left upper bronchus b1+b2+b3 (resembling the more frequent presentation of the right upper bronchus). These variants were observed in only a few patients (3.9%). Both are portrayed in Fig. 1C1 and C2, respectively). Lower lobes were second in the percentage of variations observed (Table 2 and Fig. 1B and D). Again, the right lung was more prone to anatomical variations (15% versus 11.7%). Middle lobe and lingula presented no variations.
Systematic classification of the variants observed and their relative frequencies.
| Number of observations | % of total of patients | % of total of variations observed | |
| Right lung | 57 | 31.6 | 64.7 |
| Right upper lobe | 30 | 16.6 | 34 |
| Bifurcation b1+2; b3 | 12 | 6.6 | 13.5 |
| Bifurcation b2+3; b1 | 6 | 3.3 | 6.8 |
| Bifurcation b1+3; b2 | 5 | 2.8 | 5.7 |
| Bifurcation b2+b1b; b3+b1a | 2 | 1.1 | 2.3 |
| b3 emerging directly from C | 3 | 1.7 | 3.4 |
| B emerging directly from the trachea | 2 | 1.1 | 2.3 |
| Middle lobe | 0 | 0 | 0 |
| Right lower lobe | 27 | 15 | 30.7 |
| Sub-superior bronchus | 1 | 0.6 | 1.1 |
| b7 absent | 8 | 4.4 | 9.1 |
| b7 absent: b8+B7a; b9+b7b | 2 | 1.1 | 2.3 |
| Bifurcation b8+9; b10 | 8 | 4.4 | 9.1 |
| Bifurcation b10+b9a; b8+b9b | 5 | 2.8 | 5.7 |
| Supernumerary bronchus emerging on the posterior wall of the basal pyramid | 3 | 1.7 | 3.4 |
| Left lung | 28 | 15.6 | 31.9 |
| Upper lobe division | 7 | 3.9 | 8.0 |
| Trifurcate pattern (b1+b2; b3; b4+b5) | 3 | 1.7 | 3.4 |
| Upper lobe | (4) | (2.2) | (4.5) |
| Trifurcate pattern (b1+b2+b3) | 4 | 2.2 | 4.5 |
| Lingula | (0) | (0) | (0) |
| Lower lobe | 21 | 11.7 | 23.9 |
| Sub-superior bronchus | 1 | 0.6 | 1.1 |
| Individualized b7 | 5 | 2.8 | 5.7 |
| Bifurcation b10; b9+b8 | 5 | 2.8 | 5.7 |
| Bifurcation b10+b9a; b8+b9b | 2 | 1.1 | 2.3 |
| Supernumerary bronchus emerging on the posterior wall of the basal pyramid | 8 | 4.4 | 9.1 |
| Tracheal bronchus | 3 | 1.7 | 3.4 |
 Variants observed at right upper bronchus (A1=b3 emerging directly from C; A2=Bifurcation b1+2; b3; A3 – bifurcation b2+3; b1; A4=Bifurcation b1+3; b2). (B) Variants observed at right lower lobe (B1=sub-superior bronchus; B2=supernumerary bronchus emerging on the posterior wall of the basal pyramid; B3=b7 absent). (C) Variants observed at left upper bronchus (C1=upper lobe division with a trifurcate pattern b1+b2; b3; b4+b5; C2=upper lobe with a trifurcate pattern b1+b2+b3). D) Variants observed at left lower lobe (individualized b7).")
Photographic representation of some of the anatomical variations observed. (A) Variants observed at right upper bronchus (A1=b3 emerging directly from C; A2=Bifurcation b1+2; b3; A3 – bifurcation b2+3; b1; A4=Bifurcation b1+3; b2). (B) Variants observed at right lower lobe (B1=sub-superior bronchus; B2=supernumerary bronchus emerging on the posterior wall of the basal pyramid; B3=b7 absent). (C) Variants observed at left upper bronchus (C1=upper lobe division with a trifurcate pattern b1+b2; b3; b4+b5; C2=upper lobe with a trifurcate pattern b1+b2+b3). D) Variants observed at left lower lobe (individualized b7).
Of all the variants observed, the most frequent was the presence of a bifurcate pattern (b1+2; b3) of the right upper lobe (6.6%).
A single variation was found in 64.6% of individuals while the remaining 35.4% presented two or more variations. When more than one variation was found, bilateral involvement was more frequent (67.9%).
Despite the slight predominance of variations in the male gender, no differences with statistical significance were found between the presence of variations and gender (p=0.284, Pearson's chi-square).
DiscussionThe present study represents, to the best of our knowledge, the first systematic review of the endobronchial anatomy of a Portuguese population.
Compared to the first study conducted in the Turkish population,8 our rate of endobronchial variants was very much larger (2.6% in the Turkish population and 43% in our study). The fact that our study was conducted in a prospective manner may explain the size of this difference. In fact, when compared to the second study conducted prospectively in the Turkish population,9 the frequencies observed are quite similar (42% in a sample of 1114 patients). Obviously further studies (specifically with a larger sample) are needed to ascertain a more accurate frequency of endobronchial variations within the Portuguese population.
Interestingly, the variant most frequently found within our population was the same as that observed within the Turkish population (bifurcate pattern of the right upper bronchus). Of the different patterns of right upper bronchus bifurcation, the one most frequently observed was Nagaishi's type III (b1+2; b3), which according to previous published data is not the most common bifurcation pattern.4
Although more frequent among males (as was the case in the Turkish study), no statistically significant differences were found for the presence of variations between gender.
In this study, the authors demonstrate that anatomical alternatives to the normal endobronchial branching pattern are frequent and diverse and that every bronchologist should be aware of this, when inspecting the bronchial tree, when preparing endobronchial techniques or during surgical procedures.
Conflicts of interestThe authors declare they have no conflicts of interest.
The authors wish to thank the patients for their participation in the study. Technical and operational support was gently provided by the nurses and operational assistants devoted to the bronchology unit, to whom we would also wish to show our appreciation.
Please cite this article as: Vaz Rodrigues L. Anatomia endobrônquica: estudo prospectivo das variações anatómicas da árvore traqueobrônquica. S0873-2159(11)00074-2.


