

Non-invasive mechanical ventilation (NIV) was originally used in patients with acute respiratory compromises or exacerbations of chronic respiratory diseases as an alternative to intubation. Over the last thirty years NIV has been used during the night in patients with stable chronic lung diseases such as obstructive sleep apnea, the overlap syndrome (COPD and obstructive sleep apnea), neuromuscular disorders, obesity-hypoventilation syndrome and in other conditions such as sleep disorders associated with congestive heart failure.
In this review we discuss the different types of NIV, the specific conditions in which they can be used as well as the indications, recommendations, and evidence supporting the efficacy of NIV.
A ventilação mecânica não invasiva (VNI) foi originalmente usada em doentes com insuficiência respiratória aguda ou em exacerbações de doença respiratória crónica, como uma alternativa à intubação. Nos últimos trinta anos, a VNI tem sido usada durante a noite, em doentes com doenças pulmonares crónicas estáveis, como a apneia obstrutiva do sono, a síndrome de sobreposição (DPOC - doença pulmonar obstrutiva crónica - e apneia obstrutiva do sono), disfunções neuromusculares, síndrome de hipoventilação e obesidade, e em outras doenças como os distúrbios do sono associados a insuficiência cardíaca congestiva.
Nesta análise discutimos os diferentes tipos de VNI, as condições específicas em que cada um deles pode ser usado, assim como as indicações, recomendações e a evidência que comprova a eficácia da VNI.
Noninvasive mechanical ventilation (NIV) is any form of ventilatory support without an endotracheal tube. NIV was originally used in patients with acute respiratory compromises or exacerbations of chronic respiratory diseases, as an alternative to the endotracheal tube. Over the last thirty years NIV has been also used during the night in patients with stable chronic lung disease such as obstructive sleep apnea (OSA), chronic obstructive pulmonary disease (COPD), the overlap syndrome (COPD and obstructive sleep apnea), neuromuscular disorders, obesity-hypoventilation syndrome (OHS), and sleep disorders associated with congestive heart failure (Cheyne-Stokes respiration).1,2 In this review we discuss the different types of NIV, the specific conditions in which they can be used as well as the indications, recommendations and evidence supporting the efficacy of NIV.
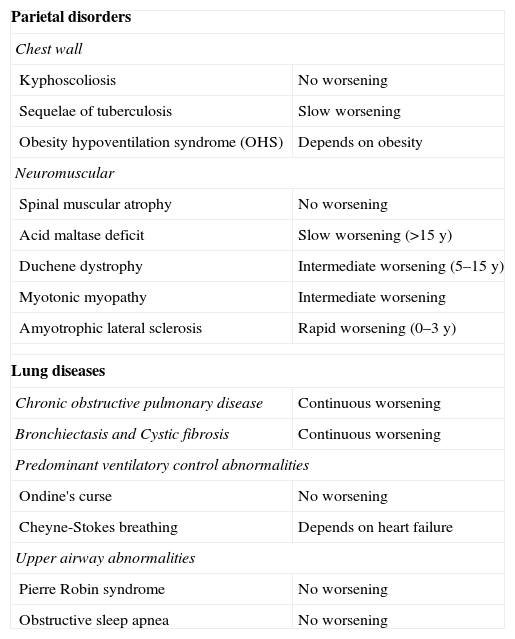
Clinical conditions for NIVAlveolar hypoventilation is a result of an imbalance between the capability of respiratory muscles to maintain ventilation and gas exchange and is characterized by hypercapnia assessed by blood gas analysis. If pathologies related to either peripheral and/or central nervous system dysfunction are excluded, the other conditions associated with developing alveolar hypoventilation are listed in Table 1.1–3 Of note, alveolar hypoventilation primarily develops during sleep4; moreover, in all these entities daytime breathing abnormalities must be considered. These respiratory “daylight” deteriorations (particularly in patients with neuromuscular disorders) require an appreciation of the diagnosis, the progression of the disease, and the particular circumstances of the patient.1–3
Main diseases which can benefit from NIV classified according the cause and progressiveness of the respiratory impairment.1,2
| Parietal disorders | |
| Chest wall | |
| Kyphoscoliosis | No worsening |
| Sequelae of tuberculosis | Slow worsening |
| Obesity hypoventilation syndrome (OHS) | Depends on obesity |
| Neuromuscular | |
| Spinal muscular atrophy | No worsening |
| Acid maltase deficit | Slow worsening (>15y) |
| Duchene dystrophy | Intermediate worsening (5–15y) |
| Myotonic myopathy | Intermediate worsening |
| Amyotrophic lateral sclerosis | Rapid worsening (0–3y) |
| Lung diseases | |
| Chronic obstructive pulmonary disease | Continuous worsening |
| Bronchiectasis and Cystic fibrosis | Continuous worsening |
| Predominant ventilatory control abnormalities | |
| Ondine's curse | No worsening |
| Cheyne-Stokes breathing | Depends on heart failure |
| Upper airway abnormalities | |
| Pierre Robin syndrome | No worsening |
| Obstructive sleep apnea | No worsening |
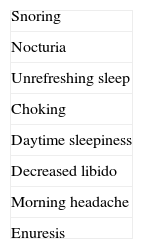
OSA has an incidence of 2% in women and 4% in men.5,6 It is characterized by recurrent episodes of partial (hypoapnea) or complete (apnea), obstruction of the upper airway during sleep, and is associated with episodes of arousal and/or oxyhemoglobin desaturation.7,8 Symptoms of the syndrome include excessive daytime sleepiness, choking episodes during sleep, frequent awakenings, unrefreshing and unstructured sleep, daytime fatigue, difficulty concentrating and short-term memory loss1 (Table 2). The pathophysiology of OSA remains controversial. Obesity, the classic hallmark in OSA, is associated with obstruction of the upper airways.9 Possible hypotheses include adipose tissue infarction of the tongue and/or the dilator muscles of the pharynx.2 The upper airway becomes less efficient, reducing oropharyngeal space especially at the end of exhalation. As a result, at the beginning of the next inspiration the dilator muscles of the pharynx must produce a greater contraction to overcome the tendency of the pharyngeal wall to collapse (due to the negative pressure inside the cavity and pharynx).7 The supine position is potentially dangerous in some circumstances8,9 because the tongue tends to occlude the rear wall of the oropharynx which can increase the oropharynx occlusion.9,10 This syndrome has been associated with the development of hypertension,11 coronary artery disease, bleeding disorders, stroke and increased risk of sudden death during sleep.12–14 It is also associated with a higher rate and greater severity of traffic accidents, increased use of health care facilities and reduced capacity for work.12,14,15 Strong evidence exists that non-invasive ventilation, usually continuous airway positive pressure (CPAP), has significant advantages in this type of disease, improving sleep quality, daytime wakefulness, and cognitive function15 and so the quality of life improves. These improvements are wide-ranging: reduction of traffic accidents, lower arterial blood pressure and reduction in the morbidity and mortality rates of myocardial infarction and stroke demonstrate the wide spectrum of CPAP's benefits.3,12,15,16
Typical symptoms of OSA.1,2
| Snoring |
| Nocturia |
| Unrefreshing sleep |
| Choking |
| Daytime sleepiness |
| Decreased libido |
| Morning headache |
| Enuresis |
We use the term “Complex Sleep Apnea” (CompSAS) to indicate a condition initially diagnosed as OSA. This syndrome is characterized (while CPAP is being used) by the frequent occurrence of central apneoa after elimination of obstructive events.17,18 CompSAS is diagnosed based on minimal apnea–hypoapnea index (AHI) of five events per hour of sleep with a majority of obstructive events. If during titration there is a reduction in the number of obstructive events to <5 events per hour of sleep, while the central apnea index (CAI) is >5 events per hour sleep, the diagnosis is established.18,19 Rather than starting further treatments it is useful to consider whether CPAP pressure is too high and is provoking CompSAS (pressure toxicity).20 Patients with CompSAS most often respond to positive airway pressure, but the obstruction cannot be eliminated without producing central apnea. A possible preventive measure is the so-called permissive flow-limitation: the pressure is set at a level that permits a mild degree of airway obstruction, without disturbing ventilator control mechanisms.17 Also oxygen administration may lead to a decrease in the hypoxic ventilatory response.17,21,22 Also BiPAP in the spontaneous-timed (ST) mode17,23 or adaptive servo-ventilation (ASV) can be useful in the treatment of CompSAS.17,18,24
Sleep-disturbances associated with cardiac dysfunctionThe prevalence of obstructive sleep apnea in patients with impaired left ventricular ejection fraction is estimated to be about 11–53%.25 It is also known that the sleep obstructive apnea–hypoapnea syndrome can worsen a state of congestive heart failure, by causing a periodic increase in negative intrathoracic pressure, by raising arterial blood pressure, and causing tachycardia from sympathetic nervous system stimulation from hypoxia, hypercapnia and arousals.26
CPAP treatment produces a reduction in blood pressure and improves left ventricular systolic function in patients with chronic heart failure and obstructive sleep apnea.11,25 Recent studies in patients with chronic heart failure associated with obstructive sleep apnea have shown a further improvement in cardiac function in patients treated with bilevel positive airway pressure ventilation (BIPAP).27 This may be due to the lower respiratory muscle work due to BIPAP. Moreover, reduced work of breathing, a lower positive intrathoracic pressure gives a greater ejection fraction.28 Central sleep apnea (CSA) is associated with periodic breathing. Periodic breathing, Cheyne-Stokes respiration, is a particular variety of central sleep apnea which is frequently associated with congestive heart failure.29 CSA with its characteristic desaturation (apnea-related) and sympathetic hyperactivity tends to worsen the prognosis of heart failure. CSA is characterized by cessation of respiratory drive during sleep, which causes impaired gas exchange.27 Unlike the OSA in which there is a respiratory effort to overcome the resistance of the upper airway, CSA is characterized by the absence of respiratory movement due to the cessation of ventilation. In the heart failure patients, the onset of apnea occurs through a redistribution of blood volume from the lower limbs to pulmonary circulation that is primarily triggered by the supine position.27,29 Stimulation of pulmonary vagal receptors causes hyperventilation which results in hypocapnia. When the value decreases below the hypocapnic apnoeic threshold, stimulation of the bulbar center ceases, inspiratory drive stops, and apnea occurs. In patients with chronic heart failure, the prolonged circulation time due to the reduction in cardiac output leads to a delay of feedback between chemoreceptors and bulbar centers resulting in hyperventilation and respiratory instability.30 The main risk factors for CSA are male sex, hypocapnia, atrial fibrillation and advanced age. CPAP and BIPAP are often unable to correct this category of apneas; therefore, a servo-assisted mode (ASV or adaptive servo ventilation) is recommended.29,31
The ASV device determinate automatically the extent of ventilatory support based on a continuous analysis of the breathing pattern and in more advanced machines also the expiratory pressure adjustment.18,24 Some studies have shown it to be most effective in controlling this type of apnea;32 it remains unclear whether ASV increases survival in these patients.33,34
Obesity-hypoventilation syndromeObesity hypoventilation refers to a syndrome including daytime hypercapnia (PCO2>45mmHg) in obese people in which no other cause of hypoventilation is present.35 Its prevalence among patients with obstructive sleep apnea is 20–30% and is greater in extremely obese patients (BMI>40).36,37 Approximately 10% of patients with obesity-hypoventilation syndrome do not have obstructive sleep apnea syndrome. Additionally, nocturnal hypoxemia and diurnal hypercapnia persist in about 40% of these patients after the treatment when CPAP eliminated apnea.35,36 Other factors contribute to the development of obesity-hypoventilation syndrome associated with the persistence of daytime hypercapnia: these include body mass index and apnea–hypoapnea index, mean overnight oxygen saturation, and the severity of restrictive ventilatory syndrome.37 CPAP treatment is most effective when there are certain predictive values: better spirometry results, and a higher apnea–hypoapnea index. BIPAP therapy may be useful in those patients for whom CPAP has failed or given unsatisfactory results. Titration of non-invasive ventilation pressure should follow the recommendations of pressure titration in obstructive sleep apnea with the goal of eliminating (hypo)apneas, snoring, respiratory effort-related arousals and lowering pCO2 levels to at least daytime values.38 No recommendations exist regarding the ventilation mode to favor in OHS.39 Trials exist providing evidence that a high backup respiratory rate leads to superior night-time control of respiratory events.40,41
The average volume-assured pressure support ventilation seems to be able to lower pCO2, but data regarding effect on oxygenation and long-term outcome are conflicting.42–45
Neuromuscular and chest wall disordersNIV has been used in patients with progressive neuromuscular disease or serious abnormalities of the thoracic cage, with recognized benefits, which include an improved survival rate and an improved quality of life. The benefits of NIV in this type of patient includes improvements of daytime levels of blood gas (including hypercapnia), a reduction in the oxygen cost of breathing, an increase in the ventilatory response to increased carbon dioxide, and improved lung compliance.46
Chronic obstructive pulmonary disease and sleep apnea (overlap syndrome)COPD is a challenging and ever increasing chronic pulmonary disease, affecting health care systems worldwide. It is projected to be fourth leading cause of mortality by 2030. COPD severely impacts quality of life.47 In severe COPD acute exacerbations often lead to acute hypoxemic and/or hypercapnic respiratory failure, resulting in further disease progression and possible chronic respiratory failure.48
NIV is considered first-line treatment in acute exacerbations of COPD requiring ventilatory support,49 but recommendations regarding establishment of domiciliary long-term non-invasive ventilation in chronic hypercapnic failure due to COPD are conflicting.50 Sleep-disordered breathing (mainly obstructive sleep apnea) and chronic obstructive pulmonary disease (COPD) are the most common lung diseases: a large number of patients have both disorders, hence the term “overlap syndrome.”51,52
The COPD overlap syndrome was first described by Flenley in 1985 as a combination of COPD and obstructive apnea–hypoapnea syndrome.53 Epidemiological studies have not shown a consistently higher incidence of sleep apnea–hypoapnea syndrome in patients with COPD compared to common OSA.52 Nevertheless, the coexistence of these conditions can lead to severe episodes of desaturation during sleep (particularly during rapid eye moviment – REM-sleep),54 thus increasing the risk of hypoxemia, daytime hypercapnia and pulmonary hypertension.55 This results in a substantially greater morbidity and mortality, compared to those with COPD or OSA alone as well as more hospitalizations and higher mortality. Many questions remain about the definition of the disease, the prognosis and the optimal treatment which currently consists of CPAP and oxygen. Non-invasive ventilation may be useful in patients with overlap syndrome, but there are no controlled studies.56,57
Clinical criteria for starting non-invasive ventilationThe presence of symptoms and physiological markers of hypoventilation are useful in identifying the clinical severity; moreover, these factors relate to therapeutic decision-making, especially initiating nocturnal non-invasive ventilation.1,2 In a typical “progressive disease” two consecutive steps occur:
- (1)
Initial phase of nocturnal hypoventilation reversible during waking hours, associated with few or no clinical symptoms.
- (2)
Nocturnal and daylight hypoventilation associated with clinical symptoms (see Table 3) which shows a reduced respiratory reserve.
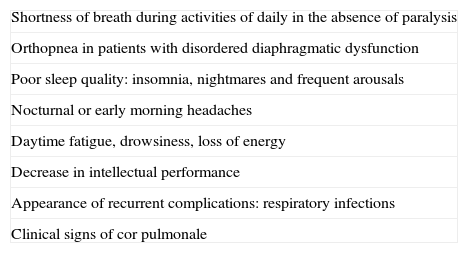
Table 3.Clinical features frequently associated with alveolar hypoventilation.1,2
Shortness of breath during activities of daily in the absence of paralysis Orthopnea in patients with disordered diaphragmatic dysfunction Poor sleep quality: insomnia, nightmares and frequent arousals Nocturnal or early morning headaches Daytime fatigue, drowsiness, loss of energy Decrease in intellectual performance Appearance of recurrent complications: respiratory infections Clinical signs of cor pulmonale
Continuous sleep monitoring of pCO2 and O2 saturation values is necessary to document the presence of nocturnal hypoventilation which may be present in all the stages of sleep (in some cases only during REM sleep). Daytime hypoventilation is defined by reduced values of arterial oxygen tension (PaO2 <55mmHg), high levels of arterial carbon dioxide tension (PaCO2 46–50mmHg) and/or high serum bicarbonate levels with a relatively normal pH. Chronic daytime hypoventilation is an important indicator always associated with nocturnal hypoventilation (PaCO2 ≥55mmHg or a rise in PtcCO2 to ≥10mmHg).52 In the presence of daytime hypoventilation, polysomnography is recommended to exclude sleep apnea.2 Clinical symptoms, although modest, should be evaluated carefully, because they are very important determining disease severity and prognosis as well defining the need for NIV. Pulmonary function tests may be helpful in defining the reduction of lung function, but they have a low predictive value for patients with sleep-related hypoventilation.2,52 However, in patients with neuromuscular disease, there is a good correlation between lung function and nocturnal hypoventilation: it has been shown that hypoventilation during REM only or during all sleep stages or in the daytime, appears respectively with supine inspiratory vital capacities of less than 40%, 25% or 12% of predicted values.1,58
Types of NIV and their useWe now consider the main types of ventilation used to treat sleep-disordered breathing and respiratory conditions associated with hypoventilation and hypercapnia.
CPAP (continuous positive airway pressure)CPAP is currently the most widely used mode of NIV in the treatment of obstructive sleep-disordered breathing59 and acute hypoxemic failure associated with chronic heart failure.59,60 It consists in the application of a constant level of positive pressure during spontaneous breathing. However, it has to be noted that CPAP should be only applied in sufficiently spontaneous breathing patients. It is not considered as a mode of mechanical ventilation.61 The mechanism of action of CPAP includes a series of actions on pathophysiological mechanisms:
- (a)
It prevents intermittent narrowing and collapse of the airways in patients with obstructive sleep apnea–hypoapnea syndrome (by acting a virtual splint during sleep).
- (b)
It counteracts auto-positive end-expiratory pressure, which reduces respiratory muscles load, the work of breathing and daytime PaCO2 in patients with overlap syndrome.
- (c)
It improves lung function, particularly the functional residual capacity, daytime gas exchange in patients with obstructive sleep apnea–hypoapnea syndrome.
- (d)
It improves systolic function of the left ventricle in patients with heart failure coexisting with obstructive sleep apnea–hypoapnea syndrome.3
Auto-CPAP (APAP) is delivered via a self-titrating CPAP device, which uses algorithms to detect variations in the degree of obstruction and adjusts the pressure level to restore normal breathing. Auto-CPAP compensates for factors that modify the upper airway collapsibility, such as body position during sleep, stage of sleep, use of alcohol, and drugs that affect upper airway muscle tone.2,3 The auto-CPAP can be used during polysomnography or cardiorespiratory monitoring to titrate a single pressure value to be used later with fixed CPAP for treatment of OSA in patients without comorbid conditions (chronic heart failure, COPD, central apnea syndrome or hypoventilation). The use of auto-CPAP is reserved only for those patients with sleep apnea syndrome only present during REM or respiratory events related to position, in whom constraining positional maneuvers are poorly tolerated.62
Adaptive servo-ventilation (ASV)The adaptive servo-ventilation (ASV) has been developed for the treatment of Cheyne-Stokes respiration-central apnea syndrome in patients with chronic heart failure who have a breathing pattern characterized by periods of crescendo–decrescendo change in tidal volume. This more complex device can use patient expiratory positive airway pressure (EPAP) level sufficient to control the obstructive apnea. The device then automatically adjusts the inspiratory pressure support for each inspiration within a pre-specified range, to maintain a moving-target ventilation set at 90% of the patient's recent average ventilation. The aim is the stabilization of breathing patterns and to reduce the respiratory alkalosis which can trigger apnea re-entry cycles.29,30,63,64
BIPAP (bilevel positive airway pressure)Bilevel positive airway pressure (BIPAP) is also used for sleep-related disorders, but its main indication is in pathological conditions associated with hypoventilation. The BIPAP devices deliver a higher pressure during inspiration (IPAP – inspiratory positive airway pressure) and a lower pressure during expiration (EPAP – expiratory positive airway pressure). The gradient between IPAP and EPAP (pressure support ventilation) is crucial in maintaining adequate alveolar ventilation and reducing paCO2.2,3 The IPAP acts also in reducing the work of breathing and fatigue, reducing the workload of respiratory muscles; EPAP has the function of maintaining the patency of the upper airway, to control obstructive apnea and to improve the functional residual capacity.3,65 BIPAP is now proposed for the type of patients who require high expiratory pressures to control obstructive sleep apnea–hypoapnea, but who cannot tolerate exhaling against a high-fixed CPAP pressure.65 Other indications of BIPAP are the treatment of coexisting central apnea or hypoventilation, the obesity-hypoventilation syndrome, the overlap syndrome and neuromuscular disorders. Although the patient should be able to maintain spontaneous breathing, it is used to set a back-up rate option for those patients whose ventilation during sleep may be particularly impaired (neuromuscular disorders, complex sleep apnea, central apnea in chronic heart failure, obesity-hypoventilation syndrome).3,65 Recently a new device has been introduced: an auto-adjusting bi-level positive airway pressure (auto-BIPAP) to provide greater flexibility in pressure changes for bi-level therapy. This treatment results in AHI (apnea–hypoapnea index) reduction equivalent to that provided by a conventional BIPAP.66
Average volume-assured pressure support ventilation (AVAPS)Average volume-assured pressure support ventilation (AVAPS) is used in patients with chronic hypoventilation and in particular with obesity hypoventilation syndrome,67 neuromuscular diseases, and sometimes, in chronic obstructive pulmonary disease. In this mode a target tidal volume is set; the device adjusts the pressure support which to reach the selected tidal volume. It guarantees a delivered tidal volume adjusted despite variability in the patient effort, airway resistance, and lung or chest wall compliance. A particular benefit of this mode is that it may be modified as the disease progresses (as it occurs in neuromuscular disorders such as amyotrophic lateral sclerosis).3 Yet, this system remains controversial. It is not known if and to what extent hybrid ventilation modes (i.e. pressure-targeted ventilation with assured volume support) are beneficial in the management of chronic hypercapnic failure. Further large-scaled studies are needed.68
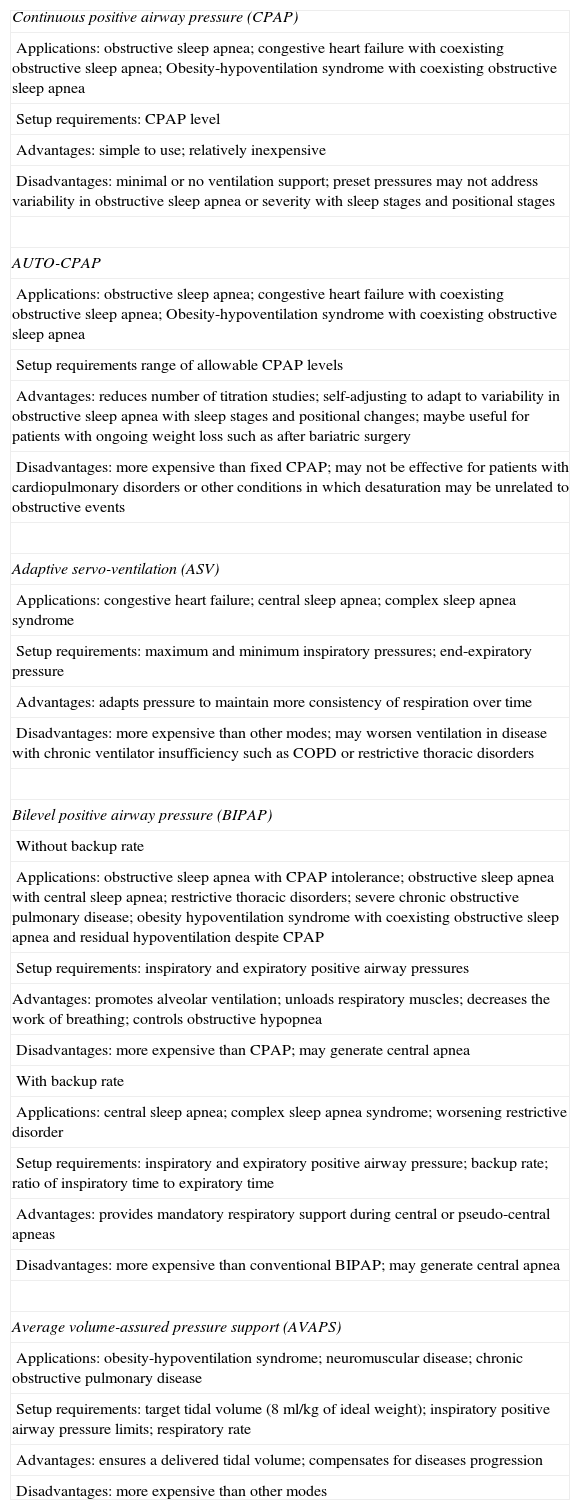
The various types of non-invasive positive pressure ventilation and their indications for the non-invasive ventilation for the various disorders are shown in Tables 4 and 5.
Types of non invasive positive pressure ventilation.3,49,50,59
| Continuous positive airway pressure (CPAP) |
| Applications: obstructive sleep apnea; congestive heart failure with coexisting obstructive sleep apnea; Obesity-hypoventilation syndrome with coexisting obstructive sleep apnea |
| Setup requirements: CPAP level |
| Advantages: simple to use; relatively inexpensive |
| Disadvantages: minimal or no ventilation support; preset pressures may not address variability in obstructive sleep apnea or severity with sleep stages and positional stages |
| AUTO-CPAP |
| Applications: obstructive sleep apnea; congestive heart failure with coexisting obstructive sleep apnea; Obesity-hypoventilation syndrome with coexisting obstructive sleep apnea |
| Setup requirements range of allowable CPAP levels |
| Advantages: reduces number of titration studies; self-adjusting to adapt to variability in obstructive sleep apnea with sleep stages and positional changes; maybe useful for patients with ongoing weight loss such as after bariatric surgery |
| Disadvantages: more expensive than fixed CPAP; may not be effective for patients with cardiopulmonary disorders or other conditions in which desaturation may be unrelated to obstructive events |
| Adaptive servo-ventilation (ASV) |
| Applications: congestive heart failure; central sleep apnea; complex sleep apnea syndrome |
| Setup requirements: maximum and minimum inspiratory pressures; end-expiratory pressure |
| Advantages: adapts pressure to maintain more consistency of respiration over time |
| Disadvantages: more expensive than other modes; may worsen ventilation in disease with chronic ventilator insufficiency such as COPD or restrictive thoracic disorders |
| Bilevel positive airway pressure (BIPAP) |
| Without backup rate |
| Applications: obstructive sleep apnea with CPAP intolerance; obstructive sleep apnea with central sleep apnea; restrictive thoracic disorders; severe chronic obstructive pulmonary disease; obesity hypoventilation syndrome with coexisting obstructive sleep apnea and residual hypoventilation despite CPAP |
| Setup requirements: inspiratory and expiratory positive airway pressures |
| Advantages: promotes alveolar ventilation; unloads respiratory muscles; decreases the work of breathing; controls obstructive hypopnea |
| Disadvantages: more expensive than CPAP; may generate central apnea |
| With backup rate |
| Applications: central sleep apnea; complex sleep apnea syndrome; worsening restrictive disorder |
| Setup requirements: inspiratory and expiratory positive airway pressure; backup rate; ratio of inspiratory time to expiratory time |
| Advantages: provides mandatory respiratory support during central or pseudo-central apneas |
| Disadvantages: more expensive than conventional BIPAP; may generate central apnea |
| Average volume-assured pressure support (AVAPS) |
| Applications: obesity-hypoventilation syndrome; neuromuscular disease; chronic obstructive pulmonary disease |
| Setup requirements: target tidal volume (8ml/kg of ideal weight); inspiratory positive airway pressure limits; respiratory rate |
| Advantages: ensures a delivered tidal volume; compensates for diseases progression |
| Disadvantages: more expensive than other modes |
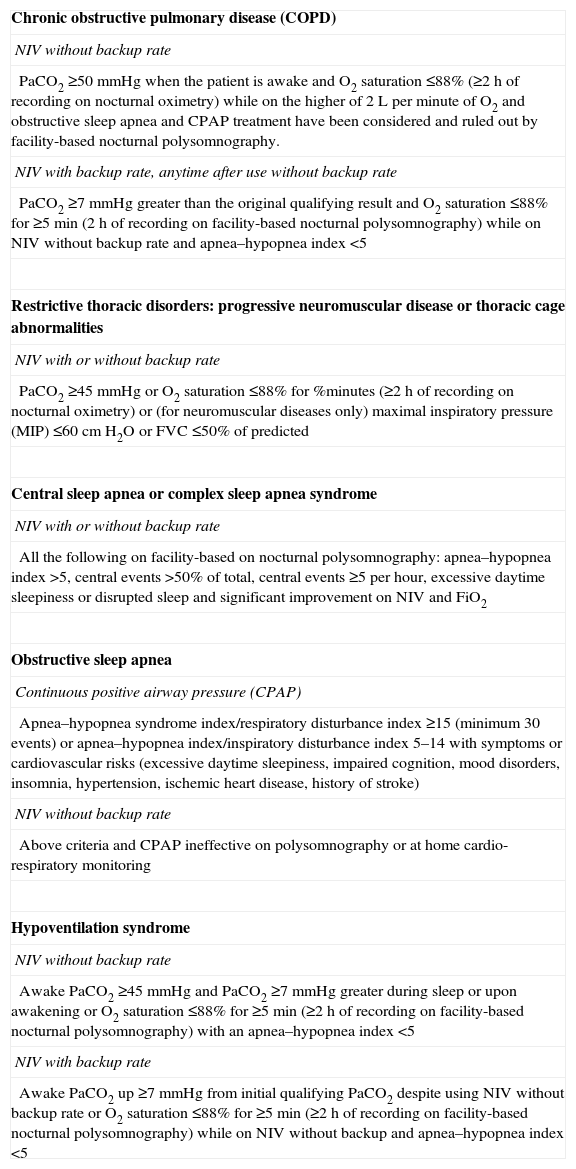
Non-invasive ventilation indication.3,49,50,59
| Chronic obstructive pulmonary disease (COPD) |
| NIV without backup rate |
| PaCO2 ≥50mmHg when the patient is awake and O2 saturation ≤88% (≥2h of recording on nocturnal oximetry) while on the higher of 2L per minute of O2 and obstructive sleep apnea and CPAP treatment have been considered and ruled out by facility-based nocturnal polysomnography. |
| NIV with backup rate, anytime after use without backup rate |
| PaCO2 ≥7mmHg greater than the original qualifying result and O2 saturation ≤88% for ≥5min (2h of recording on facility-based nocturnal polysomnography) while on NIV without backup rate and apnea–hypopnea index <5 |
| Restrictive thoracic disorders: progressive neuromuscular disease or thoracic cage abnormalities |
| NIV with or without backup rate |
| PaCO2 ≥45mmHg or O2 saturation ≤88% for %minutes (≥2h of recording on nocturnal oximetry) or (for neuromuscular diseases only) maximal inspiratory pressure (MIP) ≤60cm H2O or FVC ≤50% of predicted |
| Central sleep apnea or complex sleep apnea syndrome |
| NIV with or without backup rate |
| All the following on facility-based on nocturnal polysomnography: apnea–hypopnea index >5, central events >50% of total, central events ≥5 per hour, excessive daytime sleepiness or disrupted sleep and significant improvement on NIV and FiO2 |
| Obstructive sleep apnea |
| Continuous positive airway pressure (CPAP) |
| Apnea–hypopnea syndrome index/respiratory disturbance index ≥15 (minimum 30 events) or apnea–hypopnea index/inspiratory disturbance index 5–14 with symptoms or cardiovascular risks (excessive daytime sleepiness, impaired cognition, mood disorders, insomnia, hypertension, ischemic heart disease, history of stroke) |
| NIV without backup rate |
| Above criteria and CPAP ineffective on polysomnography or at home cardio-respiratory monitoring |
| Hypoventilation syndrome |
| NIV without backup rate |
| Awake PaCO2 ≥45mmHg and PaCO2 ≥7mmHg greater during sleep or upon awakening or O2 saturation ≤88% for ≥5min (≥2h of recording on facility-based nocturnal polysomnography) with an apnea–hypopnea index <5 |
| NIV with backup rate |
| Awake PaCO2 up ≥7mmHg from initial qualifying PaCO2 despite using NIV without backup rate or O2 saturation ≤88% for ≥5min (≥2h of recording on facility-based nocturnal polysomnography) while on NIV without backup and apnea–hypopnea index <5 |
The titration of the therapeutic value of CPAP (value of positive pressure necessary to eliminate the sleep apnea) can be made with one of the following methods:
- (1)
Sleep study with complete laboratory staff dedicated to monitoring and manual CPAP titration performed during polysomnography (the pressure is gradually increased to normalize the breathing pattern during sleep).52
- (2)
Complete polysomnographic study (with or without the continued presence of dedicated staff) with titration performed with auto-CPAP (usually the value of the 90th percentile).
- (3)
Polysomnographic full study or complete cardiorespiratory monitoring performed during nocturnal CPAP therapy whose value has been obtained on the basis of data extracted from the device auto-CPAP in the previous nocturnal recording (usually the value of the 90th percentile).
- (4)
Sleep study with complete laboratory staff dedicated to monitoring and titration of CPAP polysomnography performed in the course of using the split-night in which the patient is evaluated for 50% of the night in spontaneously breathing and the other 50% in incremental CPAP.1,69,70
Titration of PAP obtained by auto-CPAP therapy should be derived from visual analysis of a large recording period free of artifacts. The optimum pressure value of CPAP is the value which eliminates (in the course of a complete polysomnographic investigation) each apnea, hypoapnea, arterial desaturation, snoring, respiratory effort-related arousal (RERA) in each stage of sleep and body position. The same applies in the course of a complete cardiorespiratory monitoring.1,2 An acceptable level of CPAP leads to a low number of events residues during the titration procedures. The final value of pressure (PAP) is always a compromise between the function of patient adherence, the absolute value of PAP reached, and the clinical benefits derived.
It is also recommended that the procedures for titration of CPAP in points 2, 3 and 4 are made exclusively in patients with OSA in the absence of comorbidities such as COPD, chronic heart failure, and neuromuscular disorders.1,69–71
Management of non-invasive ventilationInitiation and settings in case of nocturnal ventilationThe main objective of NIV use is the correction of blood gas values to near “normal” with the least possible discomfort or sleep disturbance. It is good practice to proceed in three successive steps.1 The first step is to choose and adjust the ventilator settings while the patient is awake, assuring physiological adequacy and patient comfort for at least 1 or 2h. In the second step the clinician should evaluate the adequacy of the settings when sleeping during a nap and a night's sleep. Different options, according to the resources available in each center, are used. A full polysomnography recording oxygen saturation (SpO2) and trans-cutaneous pCO2 (PtcCO2) or end-tidal (PetCO2), flow, tidal volume, airway pressure, rib cage and abdomen excursion and sleep-staging allows a complete assessment.1,2,52 When the resources are not available fewer parameters may be used. The minimum required is recording SpO2 on room air, assessing that the normalization of SpO2 accompanies the normalization, or at least the improvement in PaCO2.
The second step relates to patient tolerance, comfort, changes in sleep quality and well-being; these data should be obtained. The third step consists of looking for reduction in PaCO2 and augmentation of PaO2 without dyspnea during the day in free ventilation after several nights of NIV. This is done to confirm that the settings are adequate for the patient's needs.1,71
The main purpose for the application of NIV is the correction of hypercapnia to physiological levels.52 Lately, a technique called “high-intensity NIV” has emerged, applying inspiratory pressure levels up to 28cm H2O and high back-up respiratory rates in order to achieve pCO2 control in stable hypercapnic COPD patients.72 This approach has been physiologically proven to reduce inspiratory effort, when compared to conventional ventilation strategies.73 Furthermore, high-intensity NIV does not negatively influence sleep quality,74 and improves blood gases, lung function, hematocrit, and decrease COPD exacerbations rates.75 However, it remains controversial what impact the setting of the breathing frequency has on ventilation quality in COPD.76
If the results are not satisfactory, changes must be made to the settings. One may also change the type of mask and ventilator. At the beginning a starting level of pressure support of 10cm H2O is recommended. Continuing the adaptation, the pressure level can progressively be increased to achieve evidence of improvement. Pressure support higher than 20cm H2O is rarely necessary.1 A back-up frequency set close to the spontaneous frequency of the patient during sleep is a reasonable step.1–3 When employing a volume-preset ventilator, the initial suggested setting may be established by adjusting the frequency of ventilator-delivered breaths so that it approximates the patient's spontaneous breathing frequency during sleep, an inspiratory time/total breathing time between 0.33 and 0.5 and a relatively high tidal volume of around 10–15ml/kg to insure sufficient tidal volume in case of leaks.1,71
Supplemental oxygen (O2) will be added to the ventilator circuit, especially in those patients who require oxygen during the daytime (COPD, cystic fibrosis, bronchiectasis). However, oxygen delivery varies greatly with the tubing system used (active valve port, leak port circuit). Furthermore, optimal mask fitting must be titrated in a clinical setting.77 In the absence of obstructive pulmonary disease, the addition of O2 to the ventilation circuit may be justified only to maintain an acceptable level of PaO2 during sleep and only after all the parameters have been optimized.78
The choice of the maskThe interface is of paramount importance for adherence to NIV therapy. The choice of this device should be done with special care to meet patient's needs. Considering the type of treatment planned and favoring masks which deliver positive pressure through both the nose and the mouth (if the patient is a mouth breather) is of great importance.79 Every effort should be made to minimize air leaks, maximize patient comfort and optimize patient–ventilator interaction.80 Technological issue to consider when choosing the NIV interface include the site and type of exhalation port, and how the ventilator algorithm functions with different masks. Heating and humidification may be needed to prevent adverse effects from cool dry gas.80,81
Continuous NIVIn patients with neuromuscular disorders (to a lesser degree in end-stage stage lung disease), ventilatory dependency can be total at the starting of non-invasive ventilation or may gradually increase following the progressive worsening of the disease. In case of continuous need for assisted ventilation, non-invasive ventilation may be started and maintained with modifications of the mode of ventilation (e.g. changing ventilation mode between day and night and/or alternating various interface types: nasal, oral, oronasal, mouth-piece) and associated, where possible, with assisted coughing.1,82
Follow-upClinical follow-up and daytime arterial blood gases should be performed at least twice a year.1,2 The recordings during sleep (possibly identical to those performed for the adaptation to non-invasive ventilation), are useful. At any time, when there are indications of unsatisfactory results such as the recurrence of clinical symptoms and/or signs of hypoventilation on arterial blood gases, inadequate non-invasive ventilation should be suspected, and a complete objective assessment of ventilation during sleep with polysomnography must be undertaken.
When the NIV is not proven to be optimal, a change of ventilation modality and/or parameters of the ventilator and/or a revision of the interface may be indicated. In case of disease progression one should be considered increasing the duration of ventilation during the day. The interfaces need to be regularly checked and modified or adapted to changing needs of the patient.1,69,71
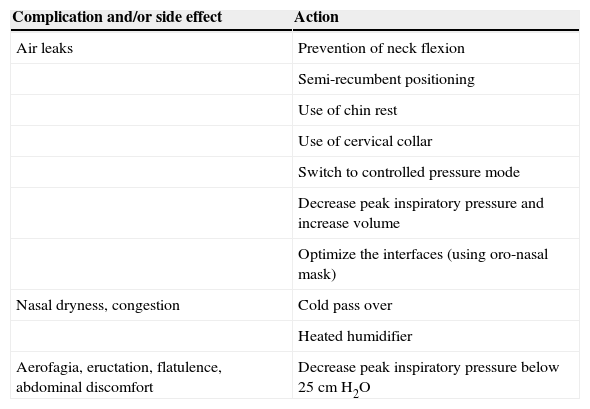
Management of complicationsAir leaks during ventilationThe major potential adverse effect is the loss of effectiveness of the ventilation and therefore the potential fragmentation of sleep. A variety of more or less effective measures have been suggested to tackle the problem of leaks during NIV. These include the prevention of neck flexion, the semi-recumbent positioning of the patient, the use of a chin rest or a cervical collar to prevent opening of the mouth, switching to controlled pressure mode, decreasing the peak inspiratory pressure and increasing the delivered volume, optimizing the interface (using full face masks if possible). The effectiveness of each of these measures must be confirmed during sleep recording.83
Nasal dryness, congestionAs shown in the CPAP literature, the side effects of nasal dryness, congestion, and rhinitis are related to a defect of humidification. For the patients with nasal and mouth dryness, a cold pass over or a heated humidifier can be used.84,85
AerophagiaAerophagia (swallowing air) is frequently reported but is rarely intolerable. Minor clinical signs are eructation, flatulence and abdominal discomfort. Aerophagia usually depends on the level of inspiratory pressure and is more common when using a volume-controlled ventilation, especially with mouthpiece, in patients with neuromuscular disorders. The incidence decreases if the peak inspiratory pressure is maintained below 25cm H2O pressure.1,85
The management of the most important complications and side effects is reported in Table 6
Management of complications and side effects of NIV.1,2
| Complication and/or side effect | Action |
|---|---|
| Air leaks | Prevention of neck flexion |
| Semi-recumbent positioning | |
| Use of chin rest | |
| Use of cervical collar | |
| Switch to controlled pressure mode | |
| Decrease peak inspiratory pressure and increase volume | |
| Optimize the interfaces (using oro-nasal mask) | |
| Nasal dryness, congestion | Cold pass over |
| Heated humidifier | |
| Aerofagia, eructation, flatulence, abdominal discomfort | Decrease peak inspiratory pressure below 25cm H2O |
Optimizing patient acceptance and adherence to non-invasive ventilation treatment is challenging and can be influenced by several factors (i.e. age, outcome expectations, leakages, and measured efficacy).86,87
Sleep-related disorders are life-threatening conditions. The optimal level of treatment should be determined in a sleep laboratory. Side effects directly affecting the patient's adherence to treatment are known. The most common are discomfort wearing the mask and leakages followed by nasopharyngeal symptoms including increased congestion and rhinorrea; these effects are related to reduced humidity of inspired gas.
Humidification of delivered gas may improve these symptoms. Sleep specialists should review the results of objective testing with the patient. Education of the patient is mandatory.
The choice of ventilator, its setting, the choice of interface between patient and ventilator are crucial for the success of NIV. A variety of masks are now available and manufacturers continue to improve mask design. Oronasal mask should be considered if the patient is mouth breather to avoid leaks through open mouth. In the past there were ventilators which had only pressure or volume controlled modes. Today most ventilators can work in either mode and the choice of the equipment should be considered by the patient's point of view. The patient's point of view is clinically relevant because better patient well-being is related to a better treatment adherence. This is a critical issue especially in patients chronically treated with non-invasive ventilation.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflicts of interestThe authors have no conflicts of interest to declare.


