

It is widely held by the scientific community that a substantial percentage of the population would need to be immune against the COVID-19 virus if we are to succeed in bringing the pandemic under control, and the safest way to achieve that objective is through a judicious, mass vaccination strategy. Within less than a year from the beginning of the COVID-19 pandemic, the collective, international efforts of the scientific community and some pharmaceutical companies have led to the development and approval of several COVID-19 vaccines. At the time of writing, numerous clinical trials have confirmed the favorable safety profile of these vaccines,1 and more than 4.51 billion individuals worldwide, equal to about 58.8 percent of the world population, have been vaccinated against the virus.2
Notwithstanding the available evidence and the overriding consensus among medical scientists about the importance and safety of COVID-19 vaccines, vaccine hesitancy, defined as “the delay in acceptance or refusal of vaccines despite availability of vaccine services”,3 has become a growing challenge for public health authorities and seems to be leading to a sub-optimal vaccination coverage in high income countries.4 The reasons underlying COVID-19 vaccine acceptance or hesitancy in the general population are unquestionably complex and not completely understood. Some of the most important factors influencing vaccine acceptance are linked to trust in science and in the information provided by health care workers and institutions, risk perception of the COVID-19 infection, and perceived vaccine safety and efficacy. Vaccination hesitancy seems to be linked to concerns about the side effects and safety of the vaccines, to the fact that they were developed in such a short period of time, and to skepticism about the benefits of this particular vaccine or of all vaccinations in general. Vaccine acceptance/hesitancy also seems to be associated with age, ethnicity, educational and income levels and marital status.5-7
In order to improve the success of COVID-19 vaccine programmes, a coordinated, evidence-based education, communication, and behavioral intervention strategy has been recently proposed, including automated reminder systems with online resources, presumptive language by health-care providers, and addressing logistical barriers to access through onsite vaccination.8
Fit, relatively young unvaccinated people account for up to 75% of subjects with COVID-19 currently being admitted to Intensive Care Units (ICUs)9: those patients unnecessarily reduce ICU bed availability and inescapably increase frontline healthcare professionals’ risk of infection. Inevitably, ICU workers may feel anger or frustration as they care for patients who could have prevented their serious health complications requiring specialized care simply by being vaccinated at the opportune time. Given these considerations, any reasonable person is prompted to wonder: were these patients unaware of the danger of refusing vaccine? Were they victims of medical misinformation? Do they change their minds/attitude about vaccination after their harrowing experience in the ICU?
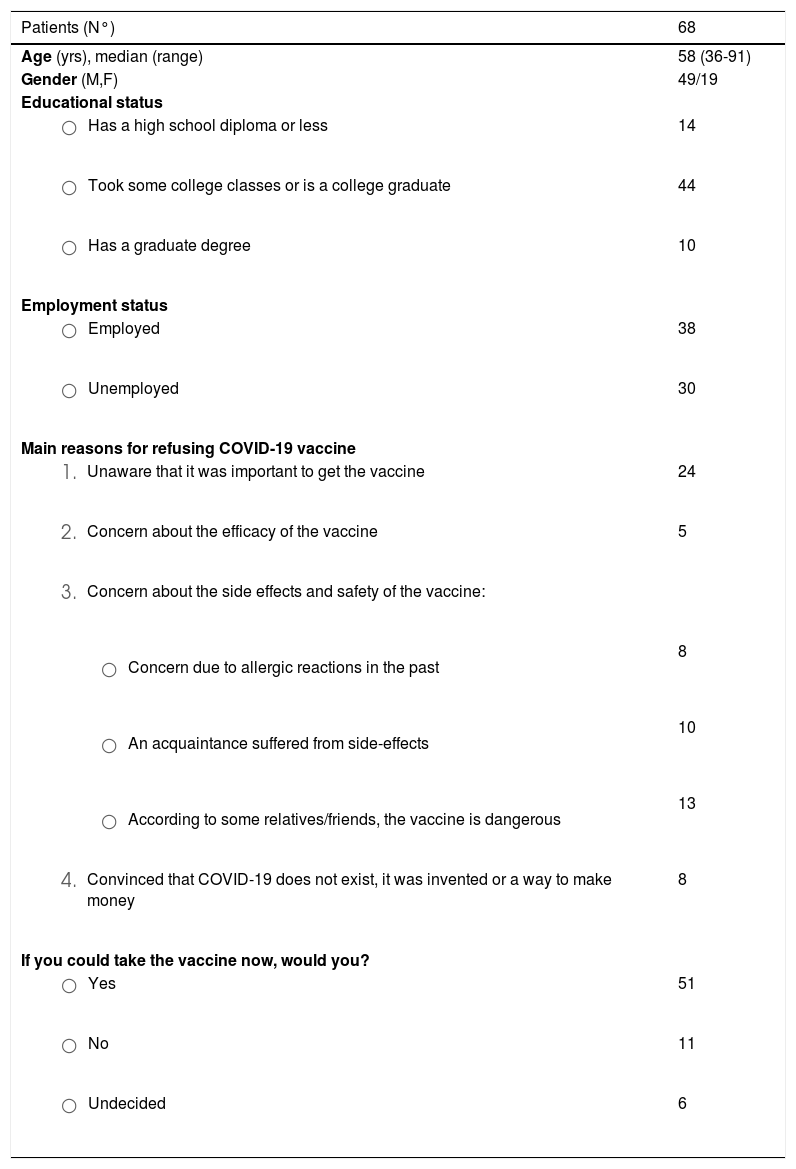
In the hopes of learning more about the real reason/s behind vaccination resistance, those of us working in the SARS-CoV-2 Respiratory ICU (RICU) of the Padova University Hospital designed a simple ad-hoc questionnaire for our patients based on a literature review of barriers to vaccination uptake.5-7,10 The questionnaire was administered by trained medical professionals (i.e., physicians, residents, and nurses) to the patients at the time they were discharged from the RICU. Out of 145 patients admitted to our RICU for severe COVID-19 from September 1st to December 15th 2021, 101 (70.1%) were unvaccinated; 68 of these agreed to fill out the questionnaire; these results (unpublished data) are outlined in Table 1.
Participants’ demographic, educational and employment characteristics, and main reasons for refusing to get COVID-19 vaccine.
An analysis of the patients’ answers suggests that vaccine refusal was driven by three main reasons: a) a lack of knowledge about the importance of receiving the vaccine against COVID-19; b) concerns about the safety of the vaccination; and c) a mixture of skepticism about orthodox medical interventions and adherence to conspiracy theories. As few individuals are untouched by the experience of requiring ICU care,11 we were expecting to see that practically all of our unvaccinated COVID-19 patients had changed their minds about the vaccine. Instead, our results demonstrated that even after their RICU experience, a significant proportion (11/68, 16.2%) still rejected vaccination.
What can we conclude from the results of our questionnaire? First, despite the efforts of international and national institutions and world-renowned scientific experts, patients still appear to be misinformed regarding the importance of COVID-19 vaccination. Second, some seem to be exceedingly worried about the vaccine's side effects, in particular they seem to fear severe allergic reactions. We would all agree that these are a more relevant barrier to vaccination than wild conspiracy theories. Third, the fact that after a frightening experience in ICU some patients are still displaying anti-vaccination attitudes could suggest that there are strong psychological barriers behind their decision.
In conclusion, although irrational arguments explain the decisions of a minority of unvaccinated patients, misinformation and lack of knowledge as well as fear appear to be the most common reasons leading to vaccination refusal in patients requiring ICU admission. Intensive care professionals need to bear this in mind to overcome frustration and not to run out of compassion for their unvaccinated patients.
We thank Sandra Marchelle for the contribution in designing the questionnaire.
Declarations of interest: None


