

Respiratory diseases (RD) constitute a significant part of the workload of family physicians. There is no consensus on what family doctors should know in this area but established methods for achieving consensus may help to overcome this.
ObjectivesThe purpose of the study was to obtain a national consensus on the required knowledge and skills in respiratory medicine for family medicine trainees after vocational training.
MethodsA Delphi study was conducted via e-mail with a diverse panel of experts. We developed a Learning Curriculum Framework (LCF) with 399 items adapted from the Royal Australasian College of Physicians ..÷ Respiratory Medicine Advanced Training Curriculum. The LCF was submitted to the experts in two rounds for consensus. Consensus was considered for items that had an agreement of 80% in the classifications above 4 on a scale of importance that ranged from 1 (not important) to 5 (very important).
ResultsConsensus was obtained for 159 items (38.8%). These included structure and function of the respiratory tract (0.6%), presenting problems (21.4%), diagnosis (7.5%), interventions and prevention (11.3%), COPD-emphysema (12.6%), tumours (3.1%), infections (10.7%), tuberculosis (5.7%), HIV (1.3%), thromboembolic disease (2.5%), pleural-pulmonary disease (3.1%), pregnancy (0.6%) and sleep disorders (3.8%). Items on iatrogenic diseases and respiratory research did not reach consensus.
ConclusionsConsensus on the respiratory medicine curriculum may contribute to further development of the vocational training curriculum in Portugal. This approach may help teachers in other countries in Europe to develop curricula for respiratory medicine and other areas of general practice.
Respiratory diseases present a challenge not only because of their high prevalence1 but also because of their impact on the health and quality of life of patients.2 They are among the leading causes of death worldwide2 and have risen to third place as a cause of death in Portugal.3 Pulmonary cancers4 and COPD5 are important causes of mortality. Asthma is also an important cause of avoidable deaths.6 RD affects all age groups and causes increased demands on health services.7 In 2011, the World Health Organization (WHO) decided that RD should be a priority and stressed the importance of prevention and control at the level of Primary Health Care (PHC).8 Primary care offers continuity of care and in the follow-up of patients, at lower costs than hospital care.9
The family medicine vocational training program is a process of specialized medical training that aims to enable physicians to practice independently in primary care.10 Throughout the course the trainee must acquire competencies that are in accordance with WONCA principles.11 It is organized over 4 years, including theoretical and practical training and on-the-job training. The objectives, divided by areas of knowledge and their complexity, should be attained by the end of the program.
There is no agreement on the relevant knowledge and skills that trainees should acquire in respiratory medicine in Portugal. Following an earlier study aimed at identifying the needs for PHC research in respiratory diseases in Portugal12 the present study aimed to develop a consensus on the knowledge and skills considered important for family physicians.
ObjectiveTo develop a national consensus on the required knowledge and skills in RD for family physicians at the end of vocational training in family medicine.
MethodsThe study used an adaptation of the Delphi methodology. This repetitive probing technique allows anonymous and systematic refining of expert opinion13 and has been used in health sciences research to obtain consensus.14 It consists of a series of rounds of information gathering to obtain a consensus in a group of experts in a given area. This can be applied to the definition of priorities, validation of clinical practices, or definition of future policies.15 In the present study, the focus was on the competencies and skills that family physicians should have in RD. A questionnaire was sent by electronic mail, which allowed for greater geographic coverage and reduced bias from in-person interviews.16...18 The research protocol was approved by the Subcommittee on Ethics for Life and Health Sciences of the University of Minho.
Selection of participantsThe panel of participants was composed of specialists in family medicine with an interest in respiratory diseases, who are part of the Respiratory Diseases Interest Group (GRESP) of the Portuguese Association of General and Family Medicine (APMGF). Additionally, specialists in family medicine with responsibilities in pre and post-graduate education, trainees who are members of GRESP and specialists in pulmonology and immuno-allergology were also invited.
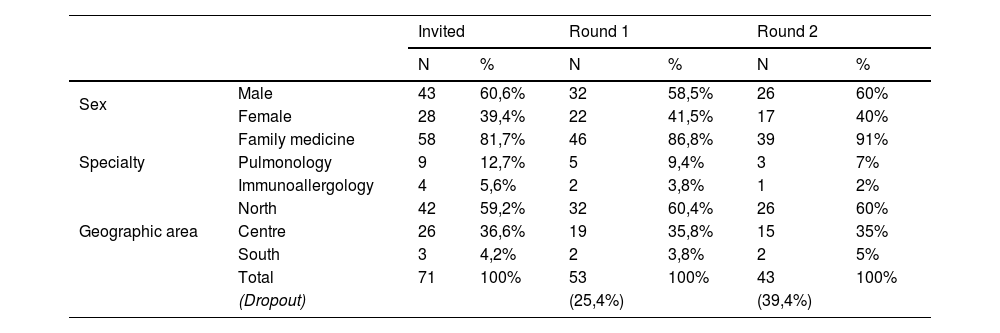
A total of 71 experts were invited to participate, of whom 43 were male (60.6%) and 28 were female (39.3%). The participants were from several districts in Portugal, including 42 from the north (59.2%), 26 from the central zone (36.6%) and 3 from the south (4.2%). Regarding medical specialties, 58 (81.7%) were specialists in family medicine, 9 (12.7%) were from pulmonology, and 4 (5.6%) were from immuno-allergology. Regarding teaching roles, 30 (42.3%) were university teachers and 26 (36.6%) were vocational training supervisors. Table 1 shows the characteristics of the participants by gender, specialty, and geographical area, and their participation in rounds 1 and 2.
Distribution of participants in rounds 1 and 2.
| Invited | Round 1 | Round 2 | |||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Sex | Male | 43 | 60,6% | 32 | 58,5% | 26 | 60% |
| Female | 28 | 39,4% | 22 | 41,5% | 17 | 40% | |
| Specialty | Family medicine | 58 | 81,7% | 46 | 86,8% | 39 | 91% |
| Pulmonology | 9 | 12,7% | 5 | 9,4% | 3 | 7% | |
| Immunoallergology | 4 | 5,6% | 2 | 3,8% | 1 | 2% | |
| Geographic area | North | 42 | 59,2% | 32 | 60,4% | 26 | 60% |
| Centre | 26 | 36,6% | 19 | 35,8% | 15 | 35% | |
| South | 3 | 4,2% | 2 | 3,8% | 2 | 5% | |
| Total | 71 | 100% | 53 | 100% | 43 | 100% | |
| (Dropout) | (25,4%) | (39,4%) | |||||
The Learning Curriculum Framework was based on the Respiratory Medicine Advanced Training Curriculum from the Royal Australasian College of Physicians.19 The final version consisted of 399 items, divided into 16 themes related to respiratory diseases. Each topic was subdivided into sections relating to knowledge, expertise, and skills. The topics included in the document were: the structure and function of the respiratory system, presenting problems, diagnosis, interventions and prevention, asthma, COPD and emphysema, tumours, pulmonary infections, tuberculosis, pulmonary manifestations of HIV-AIDS, thromboembolic and vascular disease, pleural disease, pregnancy and respiratory diseases, respiratory sleep disorders, iatrogenic respiratory diseases, and respiratory research.
The Australasian document was readily available, comprehensive and robust. It has proven its worth in practice in the setting in which it was constructed.19 It provided a convenient starting point for this study without the need to start the process from a blank canvas. The positive response to this format from the Delphi experts in this study seems to support this choice.
The original Australian document was translated from English to Portuguese and adapted by the research team, and the translation was cross-checked. The resulting document was reviewed in order to eliminate items corresponding to knowledge and skills that did not fall within the scope of family medicine. Its final wording was defined by consensus by the team. A pilot test was conducted with 7 individuals. The objective was to detect errors such as items not suitable for family medicine, repetition of items, misspellings, and errors in translation.
Delphi proceduresThe study was carried out between September and November 2017 and was conducted via electronic mail, using Google Drive.½ folders and an Excel.½ spread sheet. The statistical analysis was done on an anonymised database.20 The study consisted of two rounds of questionnaires sent to the participants. Participants had access to the results of the first round before participating in the second round.16 Communication with the participants was done through an e-mail account created for this purpose. All messages sent, as well as collected data, were reviewed by researchers to ensure clarity, simplicity and functionality of the entire process. An e-mail was sent to all potential participants, containing a brief description of the study and its objectives, inviting them to collaborate. After agreeing to participate, a code number was assigned to participants, to ensure anonymity.
In the first round, participants were asked to assess the importance of items for inclusion in the family medicine training curriculum on a five-point Likert-type scale (from 1=not important to 5=very important). The mean group responses for each item were calculated. A cut-off of 80% was chosen as the agreement value for scores of 4 and 5. Participants were asked to compare their responses from the first round to the group average and to re-assess the items. The objective was to promote reflection by the participants in order to reach consensus. At the end of the second round, the results were analyzed and the cut-off applied for consensus. Consensus was considered to have been obtained in all items that had a concordance of at least 80% for the scores of 4 or 5, on a scale of 1...5.
ResultsIn round 1, there were 53 (74.6% of all invited) participants and in round 2 there were 43 responses (81.1%). The dropout rate was 39.4% (28/71), considered acceptable given the characteristics of the method.12,14,16,20
Round 1In the first round, 3.6% of the items were considered irrelevant. All the items were included in the second round.
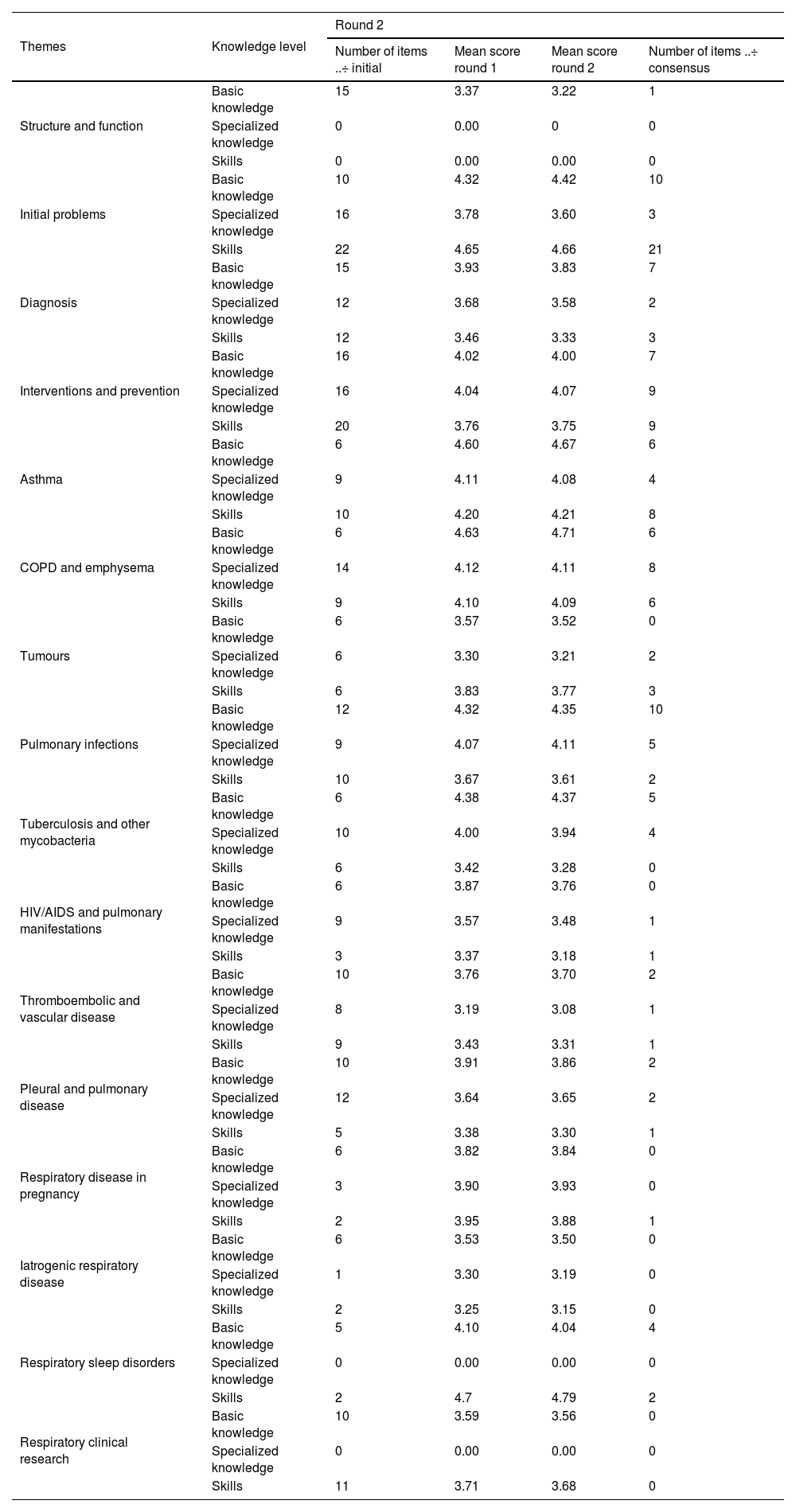
Round 2Of the 399 items in the document, 159 (38.8%) reached a level of agreement of at least 80%, with a classification of 4 or 5, on a scale of 1...5. The distribution of the items by themes was as follows : respiratory system structure and function (0.6%), presenting problems (21.4%), diagnosis (7.5%), interventions and prevention (15.7%), asthma and emphysema (12.6%), tumours (3.1%), pulmonary injuries (10.7%), tuberculosis (5.7%), pulmonary manifestations of HIV-AIDS (1.3%), thromboembolic and vascular disease (2.5%), pleural disease (3.1%), pregnancy and respiratory diseases (0.6%) and respiratory sleep disorders (3.8%). Iatrogenic respiratory diseases and respiratory clinical research did not reach consensus for any of their items. For lung manifestations of HIV-AIDS and, and respiratory disease in pregnancy, only one item had sufficient agreement. The complete analysis of all the items studied, including response averages and cut-off percentiles are available as a Supplementary file.
Table 2 lists all the items evaluated initially, as well as those that obtained consensus, distributed by themes. The averages of the responses in rounds 1 and 2 are presented for information only and did not serve as a basis for decision-making on items that met consensus. This decision was made based on the criteria described above. The proposed curriculum is available as a Supplementary file.
Items selected for inclusion in the curriculum for respiratory medicine for vocational trainees in family medicine and mean scores for items, before and after consensus by themes. Scores range from 0 to 4 on a five point Likert type scale.
| Themes | Knowledge level | Round 2 | |||
|---|---|---|---|---|---|
| Number of items ..÷ initial | Mean score round 1 | Mean score round 2 | Number of items ..÷ consensus | ||
| Structure and function | Basic knowledge | 15 | 3.37 | 3.22 | 1 |
| Specialized knowledge | 0 | 0.00 | 0 | 0 | |
| Skills | 0 | 0.00 | 0.00 | 0 | |
| Initial problems | Basic knowledge | 10 | 4.32 | 4.42 | 10 |
| Specialized knowledge | 16 | 3.78 | 3.60 | 3 | |
| Skills | 22 | 4.65 | 4.66 | 21 | |
| Diagnosis | Basic knowledge | 15 | 3.93 | 3.83 | 7 |
| Specialized knowledge | 12 | 3.68 | 3.58 | 2 | |
| Skills | 12 | 3.46 | 3.33 | 3 | |
| Interventions and prevention | Basic knowledge | 16 | 4.02 | 4.00 | 7 |
| Specialized knowledge | 16 | 4.04 | 4.07 | 9 | |
| Skills | 20 | 3.76 | 3.75 | 9 | |
| Asthma | Basic knowledge | 6 | 4.60 | 4.67 | 6 |
| Specialized knowledge | 9 | 4.11 | 4.08 | 4 | |
| Skills | 10 | 4.20 | 4.21 | 8 | |
| COPD and emphysema | Basic knowledge | 6 | 4.63 | 4.71 | 6 |
| Specialized knowledge | 14 | 4.12 | 4.11 | 8 | |
| Skills | 9 | 4.10 | 4.09 | 6 | |
| Tumours | Basic knowledge | 6 | 3.57 | 3.52 | 0 |
| Specialized knowledge | 6 | 3.30 | 3.21 | 2 | |
| Skills | 6 | 3.83 | 3.77 | 3 | |
| Pulmonary infections | Basic knowledge | 12 | 4.32 | 4.35 | 10 |
| Specialized knowledge | 9 | 4.07 | 4.11 | 5 | |
| Skills | 10 | 3.67 | 3.61 | 2 | |
| Tuberculosis and other mycobacteria | Basic knowledge | 6 | 4.38 | 4.37 | 5 |
| Specialized knowledge | 10 | 4.00 | 3.94 | 4 | |
| Skills | 6 | 3.42 | 3.28 | 0 | |
| HIV/AIDS and pulmonary manifestations | Basic knowledge | 6 | 3.87 | 3.76 | 0 |
| Specialized knowledge | 9 | 3.57 | 3.48 | 1 | |
| Skills | 3 | 3.37 | 3.18 | 1 | |
| Thromboembolic and vascular disease | Basic knowledge | 10 | 3.76 | 3.70 | 2 |
| Specialized knowledge | 8 | 3.19 | 3.08 | 1 | |
| Skills | 9 | 3.43 | 3.31 | 1 | |
| Pleural and pulmonary disease | Basic knowledge | 10 | 3.91 | 3.86 | 2 |
| Specialized knowledge | 12 | 3.64 | 3.65 | 2 | |
| Skills | 5 | 3.38 | 3.30 | 1 | |
| Respiratory disease in pregnancy | Basic knowledge | 6 | 3.82 | 3.84 | 0 |
| Specialized knowledge | 3 | 3.90 | 3.93 | 0 | |
| Skills | 2 | 3.95 | 3.88 | 1 | |
| Iatrogenic respiratory disease | Basic knowledge | 6 | 3.53 | 3.50 | 0 |
| Specialized knowledge | 1 | 3.30 | 3.19 | 0 | |
| Skills | 2 | 3.25 | 3.15 | 0 | |
| Respiratory sleep disorders | Basic knowledge | 5 | 4.10 | 4.04 | 4 |
| Specialized knowledge | 0 | 0.00 | 0.00 | 0 | |
| Skills | 2 | 4.7 | 4.79 | 2 | |
| Respiratory clinical research | Basic knowledge | 10 | 3.59 | 3.56 | 0 |
| Specialized knowledge | 0 | 0.00 | 0.00 | 0 | |
| Skills | 11 | 3.71 | 3.68 | 0 | |
This study was designed to develop a national consensus on the knowledge and skills that family physicians must acquire in respiratory diseases by the end of vocational training. Broader subjects such as the importance of multi-morbidity and polypharmacy, or the importance of psychosocial factors in respiratory diseases, are already an important part of vocational training in family medicine in Portugal.21...23
Using the Delphi method, 159 items (38.8% of the original 399 items) grouped in 14 themes, were identified by consensus of a panel of experts. Half of the total number of items included in the curriculum belonged to the themes ..úpresenting problems..., ..úinterventions and prevention... and ..úasthma and emphysema... (12.6%).
External validityThe European Academy of Teachers in General Practice/Family Medicine (EURACT), through its Educational Agenda,24 proposes a reference tool for the various teaching and training programs of family medicine at European level. In addition to defining core competencies for a family physician, it also proposes the best teaching strategies and how and where they should be taught. In addition to describing learning objectives in primary health care management, it encompasses the competencies required for a patient-centred, holistic, comprehensive and community-oriented approach. However, this document does not focus specifically on the knowledge and skills of each group of diseases.
The Portuguese training portfolio in family medicine25 is a support tool for guidance and evaluation of trainees in family medicine. It is organized by knowledge, attitudes, and skills and is assumed to be a dynamic and evolving document, adaptable to the needs of the specialty and sensitive to the contributions of all who are involved in it. It addresses the core competences of family medicine. For RD, learning objectives for knowledge, attitudes and skills are generally well established. However, the document does not specify, for each disease, what is essential to know. In addition, it is not used homogeneously throughout the country. In other European countries, the reality is similar.26,27 Learning curricula are divided into two major areas, one of which is composed of core or core competencies, and the other is dedicated to the competencies of clinical areas. The Spanish26 and English.27 experiences are worth noting. The Spanish portfolio is similar to the Portuguese portfolio. It lists objectives, but does not explore the components of each of them. One of the objectives is that the trainee must ..úknow how to carry out the approach to smoking cessation...,26 however, it does not state the skills that are required in order to implement smoking cessation. The Portuguese portfolio requires the trainee to attend at least 5 smoking cessation consultations with a tutor and then to conduct one independently. The present study included 11 items on smoking and smoking cessation (5 of specialized knowledge and 6 of competences) and all of them reached a high degree of agreement. Objectives require defined knowledge and skills with greater specificity. In the United Kingdom, the objectives are organized into 12 core competencies consisting of different items depending on the clinical module in question.28 For respiratory health, emphasis is placed on disease management including interpretation of data from the clinical history, physical examination and pulmonary function tests, leading to correct diagnosis and proper treatment. It emphasizes the effect that the personal experiences of the physician can have on patients... approach, as well as communication, ethical aspects, and teamwork within a health system. The objectives are presented in a detailed way, specifying some competences, but not stating the desired level of detail.
Internal validityThe present study identified the specific knowledge and skills to be acquired and that are omitted from other national portfolios. For asthma there was a high degree of agreement regarding certain competences such as developing management plans and writing written action plans for the patient. All the competences related to the diagnosis, treatment and education of the patient were also considered important. There was consensus on the importance of ordering, and interpretation of diagnostic tests (e.g. spirometry or cutaneous allergic tests) though it was not considered important for the family doctor to conduct these tests alone. This is consistent with the current training portfolio.
This study also identified conditions not mentioned in the portfolio such as the pulmonary manifestations of HIV/AIDS, thromboembolic disease, and sleep disorders. There was no consensus on the importance of items related to respiratory clinical research. However, the ability to critically interpret research on respiratory diseases was close to reaching consensus. Teaching research skills during training in family medicine is an idea that is gaining popularity in many countries in Europe.29 Iatrogenic respiratory disease also did not reach consensus on any of its items.
No analysis was made of the reasons participants included or excluded items. However, a reflection on the excluded set of items suggests that knowledge and skills learned during basic medical education (e.g. anatomy and physiology, RD in pregnancy, thoracic tumours and their differential diagnosis, staging, treatment and prognosis) do not need to be included in vocational training. The competences of other health professionals, such as nurses or cardio-respiratory technicians (e.g. conducting tests and examinations like spirometry) may also have been excluded. Further study is needed to clarify this.
ConclusionThe present study obtained consensus on 159 items considered important in the area of the respiratory diseases for trainees in family medicine. This study may contribute to the inclusion of additional items of knowledge and skills related to RD to the family medicine curriculum. It may encourage discussion of teaching of family medicine in Portugal. It may provide decision makers with awareness of the knowledge and skills to be acquired during vocational training.
The authors will use the content of this consensus document to make proposals to the directors of the vocational training program in family medicine in Portugal on the knowledge and skills that family physicians must have in respiratory medicine when they finish vocational training. Many of these learning and skills objectives are already part of the training program. The authors believe that the additional suggestions to be included are achievable within the present framework of vocational training.
The study is relevant to teachers of family medicine in other countries in Europe as well. Existing documents like the EURACT educational agenda suggest general principles for training without listing the clinical topics to be taught, while the current study presents specific knowledge and skill items in respiratory medicine to be taught and learned. Countries with similar health care systems, similar task profiles in general practice, and similar patient needs may use these results for future development of they own programs. Subsequent research at a European level may help to clarify the impact of the respiratory educational agenda on improving the quality of care in this area.
Ethical approvalThis study was approved by the Ethics Sub-committee for the Health and Life Sciences of the University of Minho
FundingFinancial support for this work was provided by FEDER funds through the Operational Programme Competitiveness Factors ..÷ COMPETE and National Funds through FCT ..÷ Foundation for Science and Technology under the project POCI-01-0145-FEDER-007038, and by the project NORTE-01-0145-FEDER-000013, supported by Norte Portugal Regional Operational Programme (NORTE 2020), under the PORTUGAL 2020 Partnership Agreement, through the European Regional Development Fund (ERDF).
Conflicts of interestThe authors have no conflicts of interest to declare.
We would like to thank all the participants in the Delphi for their valuable contribution.
The following are Supplementary data to this article:


