

We report the case of a 51-year-old man, former smoker (30 packs/year), complaining of progressive dyspnea, which limited his capacity to work. The patient has been working in a wood charcoal manufacturing facility for the last 30 years, with an 8h daily journey, without individual protection equipment. His activity involved carrying the charcoal from inside the masonry kilns and its fragmentation, invariably with heavy exposure to dense smoke and dust.
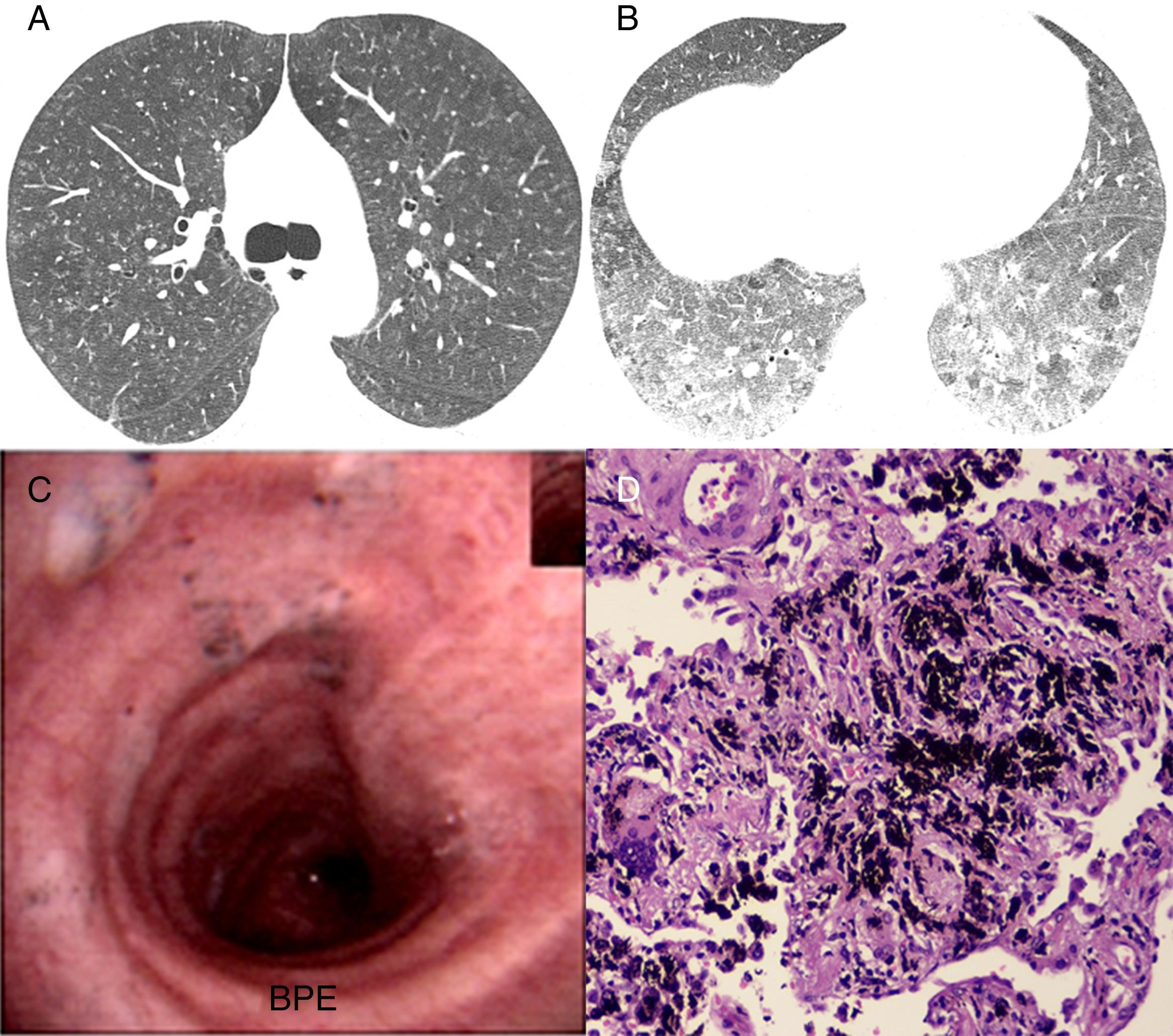
Physical examination and chest X-ray were unremarkable. A chest high resolution computed tomography (HRCT) showed diffuse ground glass opacities and ground glass centrilobular opacities, besides lobular air trapping on the expiratory acquisition (Fig. 1A and B). Bronchoscopy revealed small amount of clear mucus with black anthracotic dots on trachea and main bronchi (Fig. 1C). In a transbronchial biopsy, abundant anthracotic pigment was observed within alveolar lumen, in some macrophages and alveolar septa, without significant inflammatory or fibrotic findings (Fig. 1D). A diagnosis of wood charcoal dust related pneumoconiosis was confirmed based on clinical, radiologic and pathologic correlation.
 showing extensive centrilobular ground glass opacities and diffuse ground glass. Expiratory scan (B) showing ground-glass opacities and some lobular air trapping in the lower lobes. Bronchoscopy image showing small amount of secretion with anthracotic dots on trachea and main left bronchi (C). In (D) photomicrography showing interstitial anthracosis and multinucleated giant cell (hematoxylin–eosin, 200×).")
Inspiratory high resolution computed tomography axial scan (A) showing extensive centrilobular ground glass opacities and diffuse ground glass. Expiratory scan (B) showing ground-glass opacities and some lobular air trapping in the lower lobes. Bronchoscopy image showing small amount of secretion with anthracotic dots on trachea and main left bronchi (C). In (D) photomicrography showing interstitial anthracosis and multinucleated giant cell (hematoxylin–eosin, 200×).
Wood is the biomass fuel most frequently used both as unprocessed wood and as charcoal.1 Charcoal production involves carbonization of wood in masonry kilns, usually Eucalyptus or Pinnus spp. In Brazil, some facilities utilize a poorly mechanized process, highly dependent on human labor and associated with significant occupational hazards in each stage of its manufacture.2 Wood smoke is intensely released from the kilns, and represents a complex mixture of liquid, solid and gaseous particles, irritant and genotoxic, such as nitrogen and sulphur oxides, benzene, methanol, styrene, phenols, naphthalene, aldehydes, organic acids and polycyclic aromatic hydrocarbons.2
Both superior and inferior airway symptoms have been reported, including sneezing, nasal secretion, cough, expectoration, dyspnea, wheezing and even hemoptysis related to lower airway disease.3 Rhinitis, asthma, chronic obstructive pulmonary disease and respiratory infections may be observed in such workers.3 Literature is scant concerning interstitial lung disease/pneumoconiosis related to wood charcoal dust, especially regarding the HRCT findings. De Capitani et al.4 reported 3 cases of pneumoconiosis related to wood charcoal dust and activated carbon dust exposure. In all cases, HRCT descriptions match those observed in our cases, with centrilobular ground glass nodules. Our finding of air trapping on the expiratory scan probably representing small airway disease, was not mentioned in De Capitani et al.4 report. Similar findings have been described in carbon black pneumoconiosis, related to burning of natural gas and various petroleum products, with diffuse centrilobular ground glass nodules.5 We found no other papers describing HRCT appearance on charcoal dust exposure.
Histopathological description of black pigmented macules was observed both in our patient as in two of De Capitani et al.4 patients. No significant findings of fibrosis or inflammatory disease were observed in our patient's transbronchial or surgical biopsy, supporting the non-fibrogenic nature of this pneumoconiosis.4
In conclusion, we describe clinical, tomographic and histopathologic features of this uncommon interstitial lung pneumoconiosis related to wood charcoal smoke exposure. Considering the fact that biomass fuels are broadly disseminated as energy sources, especially in developing countries, prevention strategies in charcoal manufacturing should be encouraged in order to prevent such complications.
Conflicts of interestThe authors have no conflicts of interest to declare.


