

Timely regional-specific estimates of smoking-attributable mortality (SAM) are crucial for healthcare planning and tobacco control advocacy. Currently, this information is lacking in Portugal. The aim of this study was to estimate SAM by region in 2019 among the Portuguese population aged ≥35 years.
MethodsSAM was estimated using an independent-prevalence method. Observed mortality was obtained from Portugal Statistics; lung cancer mortality rates in smokers and never-smokers from the Cancer Prevention Study I-II and updated relative risks from five contemporary US cohort studies. SAM was estimated for each NUTS-II region by sex, age, and cause of death. Crude SAM rates, sex and age-specific rates, and age-adjusted rates were calculated using the direct method.
ResultsIn 2019, tobacco consumption caused 13,847 deaths, representing 12.3% of total mortality among the Portuguese population aged ≥35 years. Of the total SAM, 71.2% occurred in men and 22.2% in those under 65 years; 42.5% was due to cancer, 35.4% to cardiovascular and metabolic diseases, and 22.2% to respiratory diseases. SAM greatly varied among regions from 2.1% in Madeira to 36.2% in the North region. In men, cancer was the leading cause of death in all regions, while in women it was cardiovascular and metabolic diseases.
ConclusionIn Portugal, tobacco-mortality burden is high and varies significantly by region, sex and age. Therefore, estimates disaggregated by sociodemographic data and region may better support decision-makers while tailoring and implementing tobacco control policies addressing health population needs. The apparent lower tobacco burden among women and in some Portuguese regions may dramatically rise in the near future. This and the high SAM in Portugal, particularly in some regions, highlights the need to accelerate tobacco control both at national and regional levels.
Worldwide, tobacco causes an overwhelming health burden, killing more than 8 million people every year and devastating economies by increasing health costs and reducing productivity.1 Smoking affects the entire body, causing and/or aggravating non-communicable diseases (NCDs), mainly cancer, respiratory and cardiovascular diseases (CVDs).2 Likewise, tobacco increases the risk and severity of communicable diseases: tuberculosis, pneumonia and other respiratory infections.1,2 In 2019, 65% of total mortality occurring among Portuguese population was caused by three main NCD-groups: 29.9% due to CVDs, 26.0% due to tumors, and 10.9% due to respiratory diseases.3
Portugal has endorsed the World Health Organization (WHO) NCD-Global action plan, where reducing tobacco consumption is a main target;4 later reinforced by the Sustainable Development Goals aiming to strengthen the implementation of the WHO-Framework Convention on Tobacco Control (WHO-FCTC).5 In order to enhance tobacco control, WHO launched the MPOWER strategy, a package of 6 WHO-FCTC policies, where M represents tobacco epidemic monitoring, with smoking prevalence and smoking-attributable mortality (SAM) as main indicators.6
In Portugal, smoking prevalence monitoring from the National Health Survey, irregularly repeated from 1987, only includes the Azores and Madeira regions since 2005–2006.7 Regarding the tobacco epidemic, Portugal has been lagging behind due to cultural/socioeconomic determinants that prevented smoking among lower socioeconomic groups and women, preserving a lower overall smoking prevalence than most European countries.8 Over time, smoking has been declining among Portuguese men, whereas among women it increased sharply up to 2014, and decreased afterwards.8–10 However, smoking trends significantly vary by region contributing to regional health inequalities.10 During 2014–2019, Algarve presented the largest relative decrease in consumption (−23.8%) while Alentejo the smallest (−10.3%).10
The national tobacco control program (NTCP) regularly updates overall SAM by sex and specific diseases, using data from the Global Burden Disease Study (GBDS).10 Few studies have estimated SAM in Portugal,11–13 the most commonly estimated was lung cancer (LC) attributable-mortality;12,13 none have included new diseases recently attributable to tobacco consumption nor estimated SAM by region.
Although designed at national level, one of the NTCP goals is to reduce regional inequalities.10 While policy implementation should respond to population health needs, information on tobacco health burden by region is limited in Portugal.
Therefore, the aim of this study is to estimate SAM by region in 2019 among the Portuguese population aged ≥35 years, using the same sources of information and a common methodology.
MethodsEstimation methodAn independent-prevalence method proposed by Peto et al.14 was used to estimate SAM. This method uses LC mortality rate as an indirect marker of tobacco consumption past-exposure. SAM due to LC is estimated separately from other causes associated with tobacco.15
SAM estimates due to LC are based on the difference between the overall LC mortality rate and that of never-smokers.
SAM for all other causes is estimated in two steps. First, through the Smoking Impact Ratio (SIR):
where CLC is the LC mortality rate in the study population and NLC the LC mortality rate in never-smokers in the same population. S*LC and N*LC are the LC mortality rates in smokers and never-smokers in the reference population.
Second, population attributable fraction (PAF) is calculated as follows:
where RR refers to the smokers’ excess risk of dying from tobacco-related diseases compared to never-smokers.
Finally, SAM is obtained from the product of PAF and observed mortality.
Data sourcesObserved mortality in 2019 was obtained for each Portugal NUTS-II region (Nomenclature of Territorial Units for statistics II: North, Center, Lisbon metropolitan area (LMA), Alentejo, Algarve, the Azores and Madeira) from Statistics Portugal3,16 by cause of death, according to the 10th edition of the International Classification of Diseases, and by sex and age-group. Causes of death included are those with an established causal relationship with tobacco consumption according to the Surgeon General 2014-Report2 (Supplementary material Table A.1).
For each NUTS-II region, Portugal 2019 population-data was obtained from Statistics Portugal by sex and age-group.17
LC mortality rates for smokers and never-smokers in the reference population were obtained from the Cancer Prevention Study Cohorts I-II.18 LC mortality rates in never-smokers in Portugal are assumed to be equal to those of the reference population.
The relative risks (RR) among smokers compared to never-smokers from causes associated with tobacco were obtained from a pooled follow-up analysis of 956,756 patients enrolled in 5 cohort studies in the United States (US)2 (Supplementary material Table A.1).
AnalysisSAM was estimated for each specific cause and subsequently grouped into three major causes of death —cancer, cardiovascular and metabolic diseases (CVMD), and respiratory diseases—by sex, age-group (35–54, 55–64, 65–74, and ≥75 years), and NUTS-II region; i.e., the basic regions for the application of regional policies.
For each NUTS-II region, crude SAM rates, age-specific rates, and age-adjusted rates were calculated for each sex. The adjusted rates were obtained by applying the direct method with the standard European population proposed by the Eurostat's Task Force based on projections from 2011 to 2030.19
Statistical analyses were performed using Stata v.16.120 and maps with the software R.21
ResultsIn 2019, tobacco consumption caused an estimated 13,847 deaths in Portugal, 9859 (71.2%) in men and 3988 in women, accounting for 12.3% of all deaths (men: 17.6%; women: 7.1%) occurring in Portuguese adults aged ≥35 years. Of the total SAM, at least 22.2% were premature deaths occurring in those under 65 years, comprising 20.7% of the total observed mortality in that age group (35–64 years). Cancer accounted for 42.5% of total SAM, followed by CVMD (35.4%), and respiratory diseases (22.2%).
Data broken down by NUTS-II regions show that the PAF ranges from 17.4% in center to 40.1% in the Azores region. The Azores has the highest PAF both in men and women (52.7% and 26.8%, respectively); while the lowest was observed in the Center for men (24.1%) and in Alentejo for women (9.6%). Regardless of the cause of death and age-group, the highest sex ratios were observed in Madeira and Alentejo. Thus, for every woman who dies from smoking, three men die in Madeira and in Alentejo.
Cancer is the main cause of death in most regions, except in Madeira, where the burden of CVMD is higher, and in the Azores where no differences were observed between CVMD and cancer. According to sex, cancer is the leading cause of death among men in all regions, especially in the North (51.0%); while CVMD rank first among women, particularly in the Azores (50.7%). In men, the percentage difference between SAM due to cancer and CVMD varies widely among regions, being larger in the North and Center (20.6 and 16.4 percentage points, respectively) and smaller in Madeira and Alentejo (3.3 and 8.9 percentage points, respectively). Among women, big differences between CVMD and cancer were also observed in Madeira and the Azores (27.3 and 26.4 percentage points, respectively), while these differences were smaller in the North and LMA (12.3 and 13.3 percentage points) (calculated from Tables 1 and 2).
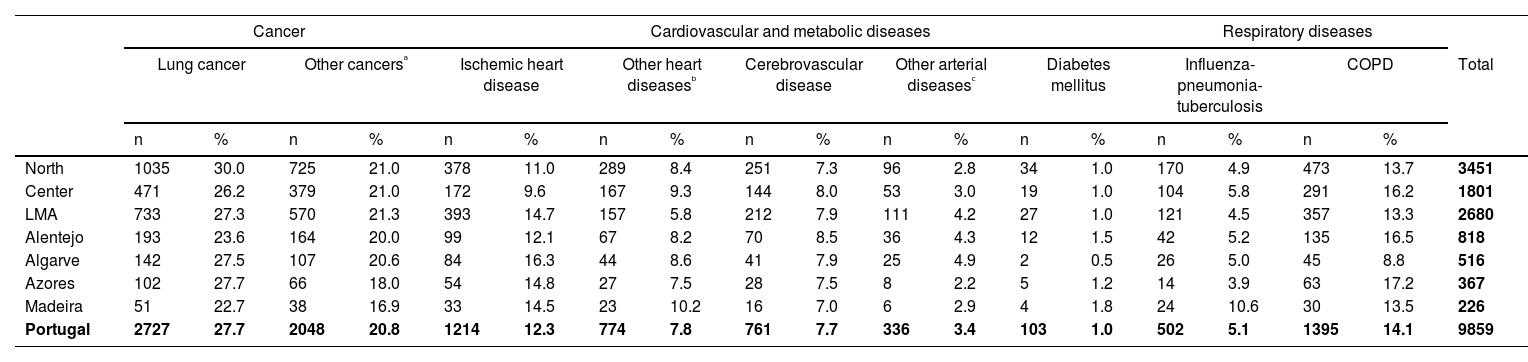
Deaths attributed to tobacco consumption and their percentage over total smoking-attributable mortality in MEN by causes of death in NUTS II regions of Portugal, 2019.
| Cancer | Cardiovascular and metabolic diseases | Respiratory diseases | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lung cancer | Other cancersᵃ | Ischemic heart disease | Other heart diseasesᵇ | Cerebrovascular disease | Other arterial diseasesᶜ | Diabetes mellitus | Influenza-pneumonia-tuberculosis | COPD | Total | ||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| North | 1035 | 30.0 | 725 | 21.0 | 378 | 11.0 | 289 | 8.4 | 251 | 7.3 | 96 | 2.8 | 34 | 1.0 | 170 | 4.9 | 473 | 13.7 | 3451 |
| Center | 471 | 26.2 | 379 | 21.0 | 172 | 9.6 | 167 | 9.3 | 144 | 8.0 | 53 | 3.0 | 19 | 1.0 | 104 | 5.8 | 291 | 16.2 | 1801 |
| LMA | 733 | 27.3 | 570 | 21.3 | 393 | 14.7 | 157 | 5.8 | 212 | 7.9 | 111 | 4.2 | 27 | 1.0 | 121 | 4.5 | 357 | 13.3 | 2680 |
| Alentejo | 193 | 23.6 | 164 | 20.0 | 99 | 12.1 | 67 | 8.2 | 70 | 8.5 | 36 | 4.3 | 12 | 1.5 | 42 | 5.2 | 135 | 16.5 | 818 |
| Algarve | 142 | 27.5 | 107 | 20.6 | 84 | 16.3 | 44 | 8.6 | 41 | 7.9 | 25 | 4.9 | 2 | 0.5 | 26 | 5.0 | 45 | 8.8 | 516 |
| Azores | 102 | 27.7 | 66 | 18.0 | 54 | 14.8 | 27 | 7.5 | 28 | 7.5 | 8 | 2.2 | 5 | 1.2 | 14 | 3.9 | 63 | 17.2 | 367 |
| Madeira | 51 | 22.7 | 38 | 16.9 | 33 | 14.5 | 23 | 10.2 | 16 | 7.0 | 6 | 2.9 | 4 | 1.8 | 24 | 10.6 | 30 | 13.5 | 226 |
| Portugal | 2727 | 27.7 | 2048 | 20.8 | 1214 | 12.3 | 774 | 7.8 | 761 | 7.7 | 336 | 3.4 | 103 | 1.0 | 502 | 5.1 | 1395 | 14.1 | 9859 |
LMA: Lisbon Metropolitan Area, COPD: chronic obstructive pulmonary disease.
Other cancers: includes lip, oral cavity and pharynx, esophagus, stomach, colon and rectum, liver and intrahepatic bile ducts, pancreas, larynx, cervix uteri, urinary bladder, kidney-renal pelvis and acute myeloid leukaemia.
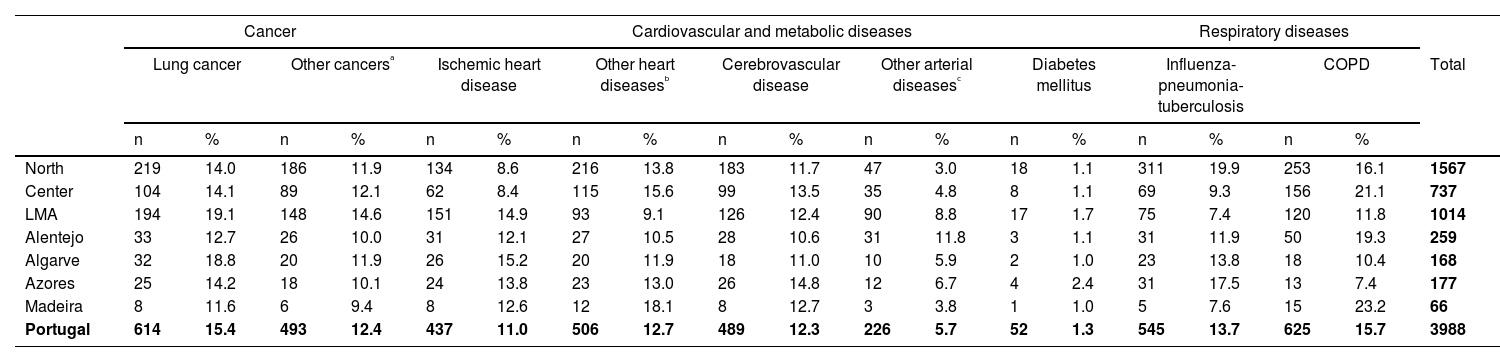
Deaths attributed to tobacco consumption and their percentage over total smoking-attributable mortality in WOMEN by causes of death in NUTS II regions of Portugal, 2019.
| Cancer | Cardiovascular and metabolic diseases | Respiratory diseases | |||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lung cancer | Other cancersᵃ | Ischemic heart disease | Other heart diseasesᵇ | Cerebrovascular disease | Other arterial diseasesᶜ | Diabetes mellitus | Influenza-pneumonia-tuberculosis | COPD | Total | ||||||||||
| n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | n | % | ||
| North | 219 | 14.0 | 186 | 11.9 | 134 | 8.6 | 216 | 13.8 | 183 | 11.7 | 47 | 3.0 | 18 | 1.1 | 311 | 19.9 | 253 | 16.1 | 1567 |
| Center | 104 | 14.1 | 89 | 12.1 | 62 | 8.4 | 115 | 15.6 | 99 | 13.5 | 35 | 4.8 | 8 | 1.1 | 69 | 9.3 | 156 | 21.1 | 737 |
| LMA | 194 | 19.1 | 148 | 14.6 | 151 | 14.9 | 93 | 9.1 | 126 | 12.4 | 90 | 8.8 | 17 | 1.7 | 75 | 7.4 | 120 | 11.8 | 1014 |
| Alentejo | 33 | 12.7 | 26 | 10.0 | 31 | 12.1 | 27 | 10.5 | 28 | 10.6 | 31 | 11.8 | 3 | 1.1 | 31 | 11.9 | 50 | 19.3 | 259 |
| Algarve | 32 | 18.8 | 20 | 11.9 | 26 | 15.2 | 20 | 11.9 | 18 | 11.0 | 10 | 5.9 | 2 | 1.0 | 23 | 13.8 | 18 | 10.4 | 168 |
| Azores | 25 | 14.2 | 18 | 10.1 | 24 | 13.8 | 23 | 13.0 | 26 | 14.8 | 12 | 6.7 | 4 | 2.4 | 31 | 17.5 | 13 | 7.4 | 177 |
| Madeira | 8 | 11.6 | 6 | 9.4 | 8 | 12.6 | 12 | 18.1 | 8 | 12.7 | 3 | 3.8 | 1 | 1.0 | 5 | 7.6 | 15 | 23.2 | 66 |
| Portugal | 614 | 15.4 | 493 | 12.4 | 437 | 11.0 | 506 | 12.7 | 489 | 12.3 | 226 | 5.7 | 52 | 1.3 | 545 | 13.7 | 625 | 15.7 | 3988 |
LMA: Lisbon Metropolitan Area, COPD: chronic obstructive pulmonary disease.
Other cancers: includes lip, oral cavity and pharynx, esophagus, stomach, colon and rectum, liver and intrahepatic bile ducts, pancreas, larynx, cervix uteri, urinary bladder, kidney-renal pelvis and acute myeloid leukaemia.
By specific causes, LC was the leading cause of death among men in all regions. By contrast, among women the leading cause differed by region: LC was the main cause of deaths attributed to tobacco consumption in LMA and Algarve, while respiratory diseases caused more deaths in the Center, Alentejo and Madeira (particularly chronic obstructive pulmonary disease); or in the North and the Azores (Tables 1 and 2).
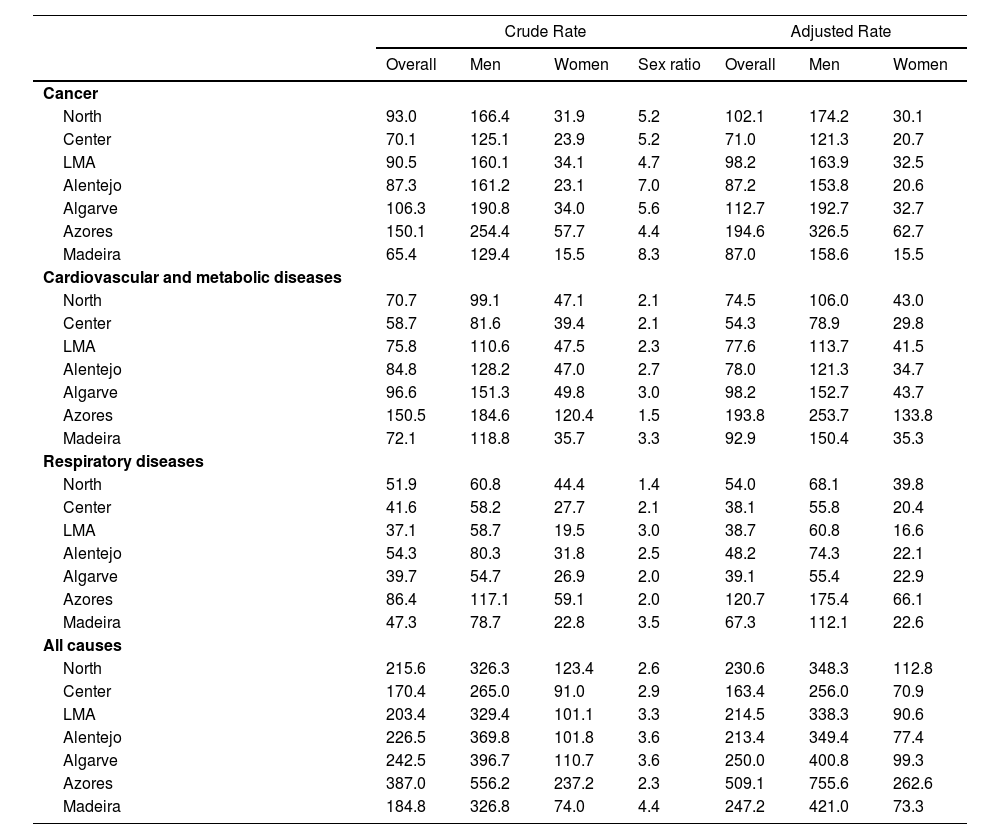
The highest SAM crude rate was observed in the Azores (387.0 per 100,000 inhabitants) and the lowest in the center (170.4 per 100,000 inhabitants). By sex, the Azores is the region with the highest SAM crude rate in both sexes (556.2 and 237.2 per 100,000 inhabitants). In contrast, the Center has the lowest crude rate in men (262.0 per 100,000 inhabitants), and Madeira the lowest in women (74.0 per 100,000 inhabitants) (Table 3).
Crude and adjusted* mortality rates for each NUTS II region of Portugal per 100,000 population in adults ≥ 35 years overall and by sex and the sex ratio of the crude rates.
LMA: Lisbon Metropolitan Area.
SAM age-specific rate increases with age among men in all regions. However, in women this pattern is observed in most regions except in Madeira, where no deaths were attributed to smoking in the 55–64 age-group (Supplementary material, Figure A.1).
For both sexes, the Azores remains the region with the highest adjusted SAM rates, while the center presents the lowest ones. Thus, the ratio of age-adjusted SAM rates between the two regions is 3 in men and 3.7 in women (Table 3).
DiscussionIn Portugal, in 2019, 12.3% of total deaths were caused by tobacco consumption. The burden of SAM is more than twofold higher in men than in women. SAM remarkably varies among regions. Cancer was the leading cause of death in men in all regions, whereas CVMD were the leading cause of death in women. The highest SAM rates were observed in the Azores in both sexes. Among men, SAM age-specific rates increased with age in all regions, although among women this pattern was not observed in Madeira.
In Portugal, 17.6% of total mortality in men and 7.1% in women in 2019 were related to tobacco consumption. This percentage is lower than those estimated in other European countries.22,23 For example, in Spain, using the same method, it was estimated that 24.2% of total mortality in men and 6.1% in women in 2017 is caused by smoking.24 These differences may be due to Portugal having an earlier tobacco epidemic stage than other European countries. Currently, Portugal seems to be the country with the lowest tobacco mortality burden, compared to other Western European countries; being in an earlier stage of the epidemic, particularly regarding women.
Lopez et al.25 in 1994, conceptualized a four-stage tobacco epidemic model in higher-income countries based on the evolution of smoking prevalence and SAM by gender, highlighting the delay between the increasingly widespread of cigarette smoking and its impact on mortality. So, SAM increases with a time gap after prevalence has increased and even sharp declines in prevalence will not be rapidly followed by SAM reduction. Later, in 2012, Thun et al26 updated the Lopez et al. tobacco epidemic model emphasizing the gender differences and saving the limitations associated with applying the Lopez model in a population in which smoking prevalence and SAM figures in women are not so high. According to the evolution of the tobacco epidemic based on Lopez model taking sex into account,25,26 Portuguese women are currently in late phase III, following the prevalence peak and still presenting low SAM. Men entered in phase IV in which prevalence is steadily decreasing but SAM has not yet started to decrease.22,23,26 Other European countries (non-EU/EEC) such as the United Kingdom or Italy, are in phase IV for both men and women, showing consistent decreases in prevalence for both sexes; while SAM among women is still rising, it is decreasing among men.23,27,28
The implementation of tobacco control policies following the ratification of WHO-FCTC, further enhanced by the NTCP activities, may have slowed the increase in smoking prevalence, particularly among women. However, in the last 30 years, Portugal has been among the Western European countries with the lowest reduction in tobacco use among men. Moreover, according to trends analysis,9,22 in Portugal the prevalence of smoking among women increased until 2014 (13.4%) and decreased until 2019 (10.9%).10
Borges et al. estimated SAM in Portugal, in 2005: 12,615 deaths were attributable to tobacco, mostly (78.4%) occurring in men, representing 11.7% of the total mortality.11 In comparison with the results found in our study, 14 years later, the percentage of SAM over the total mortality increased by less than 1% (2005: 11.7% vs. 2019: 12.3%).11 Remarkably, SAM sex disparities remained overtime; men's relative SAM has not decreased (2005: 17.7% vs. 2019: 17.6%), while women's relative SAM has increased from 5.2% (2005) to 7.1% (2019).11 SAM increase among women explains why the percentage of men's deaths upon overall SAM decreased to 71.2%. However, it should be noted that the 2005 estimate used a prevalence-dependent method and this study used a prevalence-independent method. Therefore, comparisons should be treated cautiously because the two methods use different data for the estimation of SAM. The prevalence-dependent method relies on the use of smoking prevalence, whereas the prevalence-independent method uses lung cancer mortality rates as a proxy for smoking prevalence in the past. Previous studies have indicated that the prevalence-independent method estimates a higher SAM than the prevalence-dependent one24,29 and that the greatest variation between methods occurs in groups with low smoking prevalence,24 such as Portuguese women.
According to the GBDS, using a prevalence-dependent methodology, in Portuguese women the proportion of SAM over total mortality was less than 5%, and among Portuguese men around 15–20%. In our study, similar results have been found in relation to the total mortality in men (17.6%), while in women the results are slightly higher (7.1%). Even so, these figures are lower than other Western or Southern European countries.22 However, this apparent lower tobacco mortality burden may dramatically change, since lung cancer continues to rise in Portugal, both in males and females, being the only cause of death where figures did not decrease during the recent COVID-19 pandemic.30
The Azores presents both the highest tobacco consumption and daily consumption, and the earliest age of smoking initiation;7,9,10 in this analysis it was the region with the highest SAM rates. The cause is rooted in the region. The Azores produces tobacco, and tobacco is significantly more affordable also due to a “tax benefit”. By contrast, the lowest crude SAM rates were observed in the Center, over time remaining the region with the lowest prevalence of tobacco consumption.9,10 Whereas in Madeira women have only recently started smoking,7,9 it was the only region where SAM among women did not change with age, mirroring the delayed smoking initiation by women.
Regarding the major groups of causes of death, in most regions, cancer was the leading cause, followed by CVMD. However, these differences vary among regions. Thus, the largest percentage difference between SAM due to cancer and CVMD was observed in the North region, with 10.4 percentage points (cancer: 43.1% vs. CVMD: 32.8%) and in the LMA, with 7.3 percentage points (cancer: 44.5% vs. CVMD: 37.3%). The smallest differences were observed in the Azores, where the percentage of SAM due to cancer and CVMD was similar (38.8% and 38.9%, respectively), and in Alentejo: 1.1 percentage points (cancer: 38.6% vs. CVMD: 37.4%). This highlights the inequalities in disease distribution across Portuguese regions, in line with the observed mortality: North and LMA regions present the highest percentage of mortality due to cancer, while the Azores and Alentejo the highest percentage due to CVMD.3
Regional disparities may reflect background differences in cause-specific death rates and smoking patterns; but also, the deep social and health inequalities across Portugal, particularly regarding education, income, urban/rural development, and access to health care. Portugal is one of the most unequal EU countries, with striking health inequalities.31–33 Firstly, Portugal struggles with inequalities in healthcare services provision across regions, and urban/rural areas32,34–36 LMA, center and North coastlines are wealthier urban regions, better supplied with specialized hospitals and physicians, following the higher population density.32,35,36 By contrast, the Azores and Alentejo are mostly rural and socially disadvantaged regions with significant inequalities in health care access.32,35,36 Social determinants greatly influence health literacy and health outcomes, worsening NCDs prognosis, and raising mortality risk.37 Additionally, the Azores and Alentejo present the highest smoking prevalence among men.
In Portugal, similarly to other European countries, CVD mortality has dramatically decreased (40%) due to timely diagnosis and better treatment (secondary and tertiary prevention).32 Cancer mortality also has decreased in Portugal but to a lesser extent than CVDs.3 In wealthy regions of Portugal this explains the discrepancy between SAM of cancer and CVD disease, but not in regions with low socioeconomic deprived populations with limited access to health care, such as the Azores and Alentejo.32,35,36 In these regions people with CVD do not have access to differentiated CVD care and thus, they suffer a higher mortality. In addition, unfavorable social determinants and CVD risk factors (such as high blood pressure and dyslipidemia) are less controlled in these regions due to limited access to health care.32,35,36
According to Forjaz et al.,13 the South shows the highest SAM for LC in both sexes, followed by the North. This result is also obtained in our study while combining SAM of Southern regions, i.e., Algarve and Alentejo with LMA. However, the differences between South and North regions are greater in women, with North remaining the region with the lowest smoking prevalence among women.9,10 Moreover, the highest SAM in the Southern region may result from the high smoking prevalence among women in the Algarve and LMA,9,10 mirroring different socioeconomic and cultural contexts shaping female emancipation and social roles. The wide SAM regional differences and gender disparities stress the need for further research monitoring tobacco mortality burden by region and sex among the Portuguese population.
This study has limitations mainly related to the methodology applied and data sources which should be identified.38 The independent-prevalence method uses LC as a proxy for tobacco consumption. This assumes that the disease induction time for all attributable-tobacco disorders is the same as LC. Moreover, in Portugal LC mortality rates in smokers and never-smokers, and smokers’ RR of death from smoking-related diseases compared to never-smokers are not available. Consequently, LC mortality rates and RRs derived from a different population (US), assuming that Portugal and the US share the same tobacco epidemic evolution. Additionally, this analysis neither included deaths among the population aged <35 years, nor due to secondhand tobacco smoke; underestimating the burden of disease associated with tobacco. This study also has strengths. It is pioneering while estimating SAM in Portugal NUTS-II regions for all causes of death associated with tobacco, according to the Surgeon General 2014-Report, and updating RR from five contemporary US cohorts.2 This study has used risks from a pool of 5 US cohorts in which follow-up was between 2000 and 2010, rather than using risks from the CPS-II whose follow-up was between 1982 and 1986; therefore estimates of SAM are expected to be higher because relative risks have increased.39
ConclusionsIn Portugal, smoking attributable mortality is high although remarkably varied according to sex, age-group and region. The lower burden of mortality among women and in some Portuguese regions may dramatically rise in the near future. These findings emphasize the need for strengthening tobacco control and tobacco-mortality monitoring, nationally and locally.
FundingThis research was supported by the Instituto de Salud Carlos III (ISCIII) through the project “PI19/00288″ and co-funded by the European Union.
Data statementThe datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
This paper forms part of the research for the PhD degree of Julia Rey-Brandariz, who received a FPU fellowship (reference number FPU20/00926), from the Ministry of Universities of Spain.


