


Quality of life (QOL), sexual satisfaction (SS) and physical performance have been assessed in the management of numerous chronic diseases.
MethodsIn this study, the following tests and surveys were applied: (i) QOL questionnaire [Cystic Fibrosis Questionnaire (CFQ)]; (ii) SS questionnaire (SSQ) [female sexual quotient (FSQ) and male sexual quotient (MSQ)]; (iii) 6-minute walk test (6MWT). Spearman's correlation was used for comparison between the data; the Mann–Whitney test was applied to analyze the difference between genders. A total of 52 adult patients with CF were included in this study.
ResultsThere was a positive correlation between CFQ domains and SSQ questions. The CFQ showed a positive correlation with peripheral oxygen saturation of hemoglobin (SpO2) and the distance walked in the 6MWT, and a negative correlation with the Borg scale. The SSQ showed positive correlation with the distance walked and a negative correlation with the Borg scale. For some markers evaluated in the 6MWT, there was sometimes association with the evaluated domains and questions. Male patients showed better scores in the emotional CFQ domain, better performance in SSQ and physical performance.
ConclusionsThere was a correlation between CFQ, SSQ and 6MWT in CF. Finally; we believe that QOL surveys should assess the domain “sexuality” as well as physical performance tests.
Continuous improvements in the management of cystic fibrosis (CF) allow increasing life expectancy of CF patients, who currently live well onto adulthood. Even with aggressive treatment, CF patients develop malnutrition, reduced lung function and various comorbidities, which affect physical performance and quality of life (QOL). The analysis of physical performance and QOL are important tools for clinical evaluations and individual monitoring. It measures the extent to which individuals are satisfied with their lives, assessing their cultural and social contexts, goals, expectations, standards and concerns.1
Both physical performance and QOL influence sexuality. In chronic diseases, such influences may be intensified. Studies of CF patients show that the progression of the disease leads to reduced physical performance and QOL, followed by lower sexual satisfaction.2–4
Although there are many tests to assess QOL, the Cystic Fibrosis Questionnaire, mostly used in CF, does not include the evaluation of sexuality. So, sexuality should be evaluated as part of human development, due to its relation to physical and mental health. Sexual satisfaction (SS) includes the act itself and its elements, i.e., satisfaction and desire for both sexes.
Sexual dysfunctions may occur due to lack or excess of sexual desire, discomfort and/or pain during sexual relations, which will have a negative impact on desire, arousal and/or orgasm. At times, sexual relations will be either interrupted or avoided. Therefore, sexuality also affects QOL. In chronic diseases, mutual deterioration in QOL and sexuality has proved to be associated with physical and emotional changes.3,4
Psysical performance and QOL of CF patients can affect their SS. Physical performance can be evaluated by several methods. The most commonly used test is the 6-minute walk test (6MWT), which evaluates the patient's submaximal walking performance.5
In this context, the aim of this study was to evaluate the correlation between 6MWT, QOL and SS and the differences of data between both sexes in CF adult's patients.
MethodsThis is an observational and analytical cross-sectional study, which was carried out at the Referral Center for Cystic Fibrosis.
The diagnosis of CF was made based on the clinical history compatible with CF, two sweat tests with chloride levels ≥60mEq/L and/or two identified mutations in the CFTR gene (Cystic Fibrosis Transmembrane Regulator). Patients older than 18 years and patients without pulmonary exacerbation during the study were included in order to avoid bias in the 6MWT.
Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. The study was approved by the Research Ethics Committee of the Unicamp (#756453).
CFQ and SSQ were completed and the 6MWTs were performed at the Unicamp University Hospital.
Quality of life questionnaire (QOL)The CFQ includes a total of 12 items (domains): physical role, social role, vitality, emotional state, social limitations, body image, eating disturbances, treatment constraints, health perceptions, weight, respiratory symptoms and digestive symptoms. The score of each domain ranges from zero to one hundred. The highest values are associated with better QOL scores. The score was validated for use in Brazil by Rozov et al.6 In total, 50 questions were answered by the patients and the data was entered into the software program developed by Quittner et al.,1 which generates a numerical profile for each domain.
Sexual satisfaction questionnaireThe SSQ is different for each gender [male sexual quotient (MSQ) and female sexual quotient (FSQ)] (Online Resource 1). A total of 10 questions were evaluated for each SSQ. The MSQ was validated by Abdo (2007) and includes the following domains: desire and drive; self-confidence and ejaculation; foreplay and ejaculation; desire, ejaculation and erection; desire and erection (time); desire and erection (satisfaction); desire and erection (sequence); ejaculation (control); ability to reach orgasm; and performance and SS.7 The FSQ was validated by Abdo8 and includes all questions about desire and sexual interest (questions 1, 2 and 8), foreplay (question 3); arousing of the woman and sexual interaction with partner (questions 4 and 5), comfort in sexual intercourse (question 6 and 7); orgasm and SS (questions 9 and 10). In SSQ, each question ranges from zero to five points. The SSQ score is obtained by the sum of 10 questions multiplied by two to obtain the weight average of 100. In the question seven for the FSQ, the score was already fixed, i.e., five. The score was calculated as follows: five minus the value given by the patient. In the SSQ, the following reference ranges and respective interpretative comments were observed: (i) 0–20 points – null to poor; (ii) 22–40 points – poor to unfavorable; (iii) 42–60 – unfavorable to regular; (iv) 62–80 – regular to good; (v) 82–100 – good to excellent.7,8
Six-minute walk testThe 6MWT was performed following the guidelines of the American Thoracic Society.9,10
The 6MWT is a simple, inexpensive and easily applicable method. It is a submaximal clinical exercise tolerance test, and therefore it can be performed by patients with restrictions for maximal exercise tests. 6MWTs are safer than the maximal exercise tests because patients are able to define their own limits during the exercise. The ability to walk a certain distance has a direct impact on the QOL as well as on the ability to perform daily tasks.9
This study assessed three time periods: (i) rest (period before the beginning of the test: the patient's physical condition is evaluated at rest); (ii) 6min after the beginning of test (indicative marker of patient's metabolic changes during physical exertion); (iii) 9min after completion of the test (indicative marker of patient's recovery after the physical exertion). In each period, the following markers were assessed: (i) peripheral oxygen saturation of hemoglobin (SpO2); (ii) heart rate (HR-bpm); (iii) inspiratory frequency (f – ipm); (iv) systemic arterial pressure (mmHg); (v) Borg scale; (vi) distance walked (in meters and percentage of predicted value). Other data included: (i) weight (kg); (ii) height (m); (i) body mass index (kg/m2); (iv) age (years); (v) time of the disease (years); and (vi) gender (male and female).
The Borg scale is a visual analog scale, which helps measure the degree of respiratory distress before and after the 6MWT. Its results are reproducible, they measure perceived dyspnea in adults, and assess the intensity of physical exertion. The scale consists of a horizontal line quantified from 0 to 10. Zero represents “no breathlessness” and 10 is “the most severe breathlessness”. The patient should select a single score that would reflect the degree of dyspnea.11
Statistical analysisStatistical analysis was performed using SPSS software (Statistical Package for Social Sciences) version 22.0 (IBM, São Paulo, Brazil) and graphic construction using MedCalc software version 16.2 (Microsoft®, Ostend, Belgium).
Categorical data was presented according to the proportion of patients (percentage). Numerical data was presented as frequency, mean, median, standard deviation, minimum and maximum. The correlation analysis between the CFQ, SSQ and 6MWT was performed by Spearman's coefficient (Rho) showing confidence interval of 95%CI. For the comparison between gender and CFQ, SSQ and 6MWT, the Mann–Whitney test was used for data with numerical distribution and the χ2 for data with categorical distribution. The alpha value was set at 0.05 in all analyses.
ResultsA total of 52 adult CF patients were included. Online Resource 2 shows the description of the data evaluated in the study and the distribution of QOL and SS scores of CF patients. Of these patients, 12 CF patients did not answer the SSQ because they had not started their sexual activity. However, these CF patients were enrolled in the study because they performed the 6MWT and SSQ.
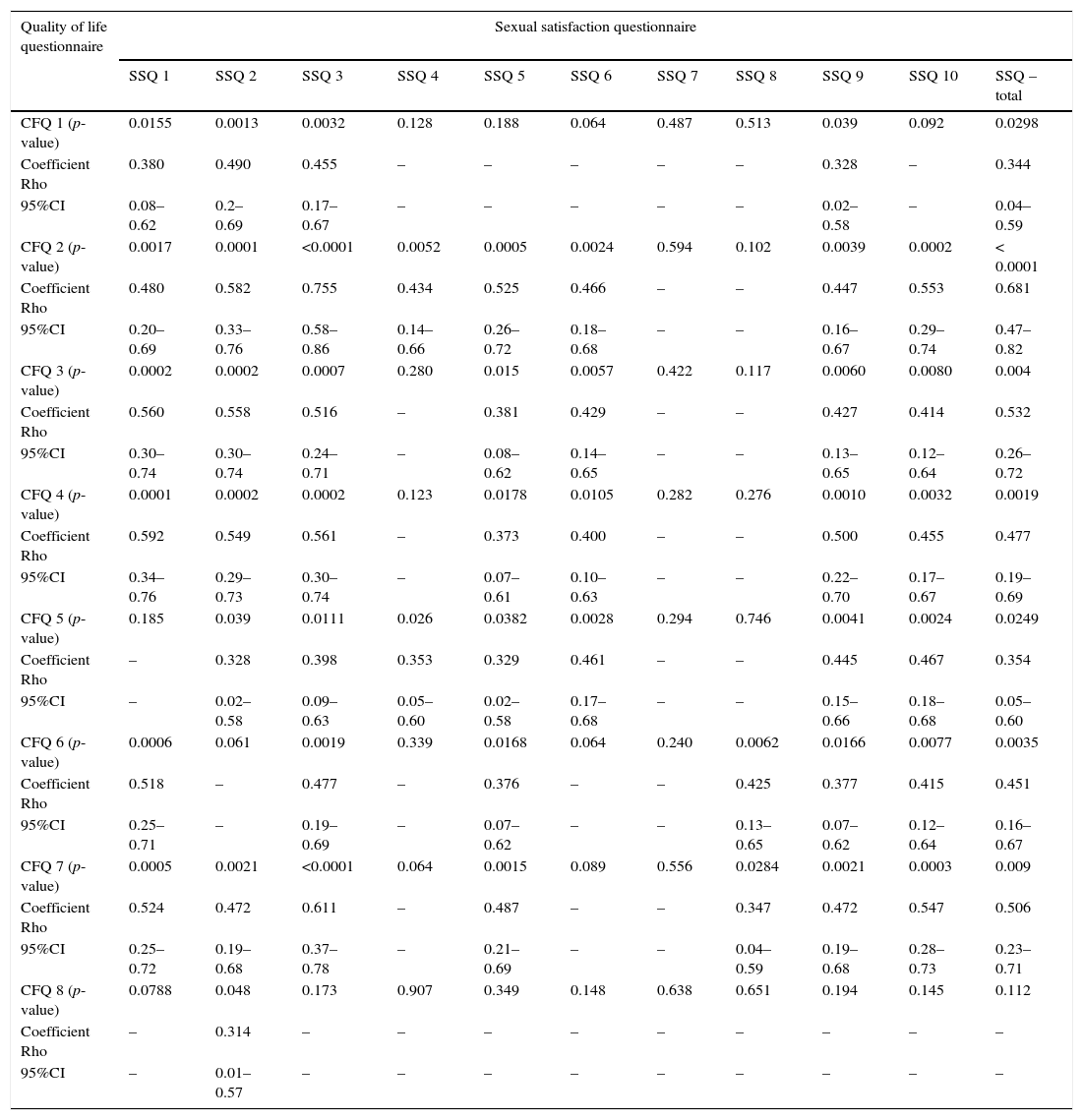
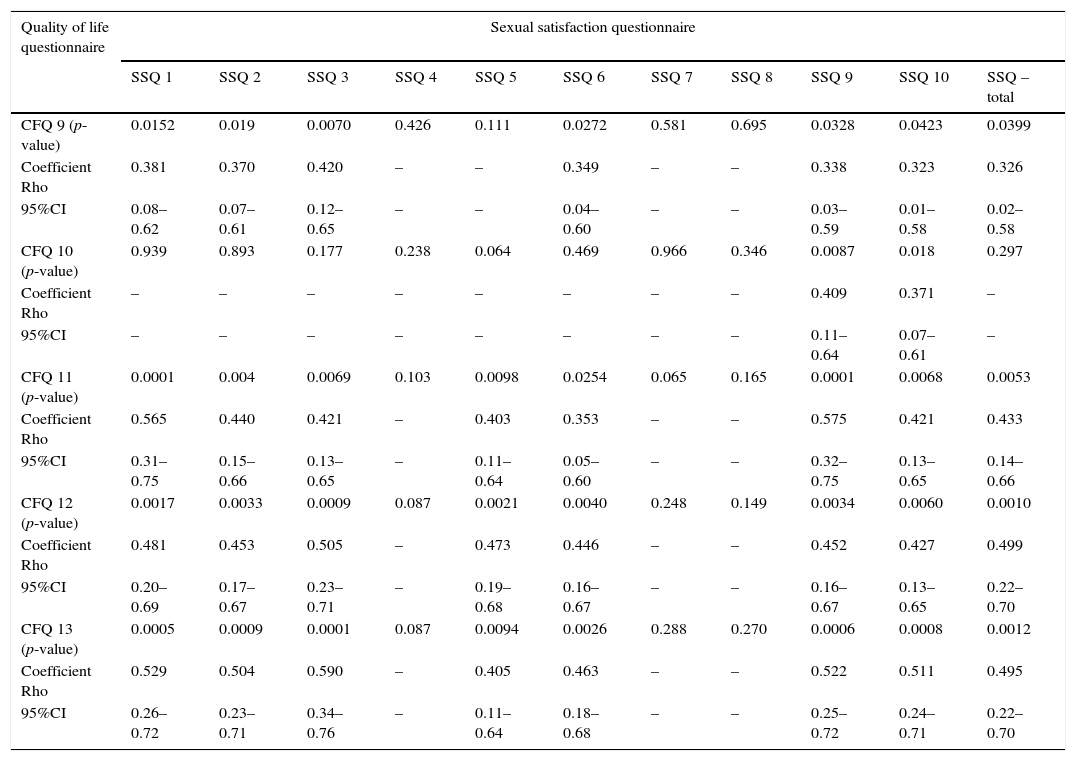
The correlation between the values of the CFQ and SSQ are presented in Tables 1A and 1B. There was a correlation between all questions of SSQ and all domains of CFQ for at least one answer, except for question 7 of SSQ.
Correlation between values of quality of life questionnaire and sexual satisfaction questionnaire in patients with cystic fibrosis (Part I).
| Quality of life questionnaire | Sexual satisfaction questionnaire | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SSQ 1 | SSQ 2 | SSQ 3 | SSQ 4 | SSQ 5 | SSQ 6 | SSQ 7 | SSQ 8 | SSQ 9 | SSQ 10 | SSQ – total | |
| CFQ 1 (p-value) | 0.0155 | 0.0013 | 0.0032 | 0.128 | 0.188 | 0.064 | 0.487 | 0.513 | 0.039 | 0.092 | 0.0298 |
| Coefficient Rho | 0.380 | 0.490 | 0.455 | – | – | – | – | – | 0.328 | – | 0.344 |
| 95%CI | 0.08–0.62 | 0.2–0.69 | 0.17–0.67 | – | – | – | – | – | 0.02–0.58 | – | 0.04–0.59 |
| CFQ 2 (p-value) | 0.0017 | 0.0001 | <0.0001 | 0.0052 | 0.0005 | 0.0024 | 0.594 | 0.102 | 0.0039 | 0.0002 | < 0.0001 |
| Coefficient Rho | 0.480 | 0.582 | 0.755 | 0.434 | 0.525 | 0.466 | – | – | 0.447 | 0.553 | 0.681 |
| 95%CI | 0.20–0.69 | 0.33–0.76 | 0.58–0.86 | 0.14–0.66 | 0.26–0.72 | 0.18–0.68 | – | – | 0.16–0.67 | 0.29–0.74 | 0.47–0.82 |
| CFQ 3 (p-value) | 0.0002 | 0.0002 | 0.0007 | 0.280 | 0.015 | 0.0057 | 0.422 | 0.117 | 0.0060 | 0.0080 | 0.004 |
| Coefficient Rho | 0.560 | 0.558 | 0.516 | – | 0.381 | 0.429 | – | – | 0.427 | 0.414 | 0.532 |
| 95%CI | 0.30–0.74 | 0.30–0.74 | 0.24–0.71 | – | 0.08–0.62 | 0.14–0.65 | – | – | 0.13–0.65 | 0.12–0.64 | 0.26–0.72 |
| CFQ 4 (p-value) | 0.0001 | 0.0002 | 0.0002 | 0.123 | 0.0178 | 0.0105 | 0.282 | 0.276 | 0.0010 | 0.0032 | 0.0019 |
| Coefficient Rho | 0.592 | 0.549 | 0.561 | – | 0.373 | 0.400 | – | – | 0.500 | 0.455 | 0.477 |
| 95%CI | 0.34–0.76 | 0.29–0.73 | 0.30–0.74 | – | 0.07–0.61 | 0.10–0.63 | – | – | 0.22–0.70 | 0.17–0.67 | 0.19–0.69 |
| CFQ 5 (p-value) | 0.185 | 0.039 | 0.0111 | 0.026 | 0.0382 | 0.0028 | 0.294 | 0.746 | 0.0041 | 0.0024 | 0.0249 |
| Coefficient Rho | – | 0.328 | 0.398 | 0.353 | 0.329 | 0.461 | – | – | 0.445 | 0.467 | 0.354 |
| 95%CI | – | 0.02–0.58 | 0.09–0.63 | 0.05–0.60 | 0.02–0.58 | 0.17–0.68 | – | – | 0.15–0.66 | 0.18–0.68 | 0.05–0.60 |
| CFQ 6 (p-value) | 0.0006 | 0.061 | 0.0019 | 0.339 | 0.0168 | 0.064 | 0.240 | 0.0062 | 0.0166 | 0.0077 | 0.0035 |
| Coefficient Rho | 0.518 | – | 0.477 | – | 0.376 | – | – | 0.425 | 0.377 | 0.415 | 0.451 |
| 95%CI | 0.25–0.71 | – | 0.19–0.69 | – | 0.07–0.62 | – | – | 0.13–0.65 | 0.07–0.62 | 0.12–0.64 | 0.16–0.67 |
| CFQ 7 (p-value) | 0.0005 | 0.0021 | <0.0001 | 0.064 | 0.0015 | 0.089 | 0.556 | 0.0284 | 0.0021 | 0.0003 | 0.009 |
| Coefficient Rho | 0.524 | 0.472 | 0.611 | – | 0.487 | – | – | 0.347 | 0.472 | 0.547 | 0.506 |
| 95%CI | 0.25–0.72 | 0.19–0.68 | 0.37–0.78 | – | 0.21–0.69 | – | – | 0.04–0.59 | 0.19–0.68 | 0.28–0.73 | 0.23–0.71 |
| CFQ 8 (p-value) | 0.0788 | 0.048 | 0.173 | 0.907 | 0.349 | 0.148 | 0.638 | 0.651 | 0.194 | 0.145 | 0.112 |
| Coefficient Rho | – | 0.314 | – | – | – | – | – | – | – | – | – |
| 95%CI | – | 0.01–0.57 | – | – | – | – | – | – | – | – | – |
CFQ, quality of life questionnaire for cystic fibrosis; SSQ, sexual satisfaction questionnaire; 95%CI, confidence interval of 95%. Sample size=40. Spearman's coefficient (Rho) was used for statistics, with confidence interval of 95%. Only coefficients of positive associations are demonstrated. α=0.05.
Correlation between values of quality of life questionnaire and sexual satisfaction questionnaire in patients with cystic fibrosis (Part II).
| Quality of life questionnaire | Sexual satisfaction questionnaire | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| SSQ 1 | SSQ 2 | SSQ 3 | SSQ 4 | SSQ 5 | SSQ 6 | SSQ 7 | SSQ 8 | SSQ 9 | SSQ 10 | SSQ – total | |
| CFQ 9 (p-value) | 0.0152 | 0.019 | 0.0070 | 0.426 | 0.111 | 0.0272 | 0.581 | 0.695 | 0.0328 | 0.0423 | 0.0399 |
| Coefficient Rho | 0.381 | 0.370 | 0.420 | – | – | 0.349 | – | – | 0.338 | 0.323 | 0.326 |
| 95%CI | 0.08–0.62 | 0.07–0.61 | 0.12–0.65 | – | – | 0.04–0.60 | – | – | 0.03–0.59 | 0.01–0.58 | 0.02–0.58 |
| CFQ 10 (p-value) | 0.939 | 0.893 | 0.177 | 0.238 | 0.064 | 0.469 | 0.966 | 0.346 | 0.0087 | 0.018 | 0.297 |
| Coefficient Rho | – | – | – | – | – | – | – | – | 0.409 | 0.371 | – |
| 95%CI | – | – | – | – | – | – | – | – | 0.11–0.64 | 0.07–0.61 | – |
| CFQ 11 (p-value) | 0.0001 | 0.004 | 0.0069 | 0.103 | 0.0098 | 0.0254 | 0.065 | 0.165 | 0.0001 | 0.0068 | 0.0053 |
| Coefficient Rho | 0.565 | 0.440 | 0.421 | – | 0.403 | 0.353 | – | – | 0.575 | 0.421 | 0.433 |
| 95%CI | 0.31–0.75 | 0.15–0.66 | 0.13–0.65 | – | 0.11–0.64 | 0.05–0.60 | – | – | 0.32–0.75 | 0.13–0.65 | 0.14–0.66 |
| CFQ 12 (p-value) | 0.0017 | 0.0033 | 0.0009 | 0.087 | 0.0021 | 0.0040 | 0.248 | 0.149 | 0.0034 | 0.0060 | 0.0010 |
| Coefficient Rho | 0.481 | 0.453 | 0.505 | – | 0.473 | 0.446 | – | – | 0.452 | 0.427 | 0.499 |
| 95%CI | 0.20–0.69 | 0.17–0.67 | 0.23–0.71 | – | 0.19–0.68 | 0.16–0.67 | – | – | 0.16–0.67 | 0.13–0.65 | 0.22–0.70 |
| CFQ 13 (p-value) | 0.0005 | 0.0009 | 0.0001 | 0.087 | 0.0094 | 0.0026 | 0.288 | 0.270 | 0.0006 | 0.0008 | 0.0012 |
| Coefficient Rho | 0.529 | 0.504 | 0.590 | – | 0.405 | 0.463 | – | – | 0.522 | 0.511 | 0.495 |
| 95%CI | 0.26–0.72 | 0.23–0.71 | 0.34–0.76 | – | 0.11–0.64 | 0.18–0.68 | – | – | 0.25–0.72 | 0.24–0.71 | 0.22–0.70 |
CFQ, quality of life questionnaire for cystic fibrosis; SSQ, sexual satisfaction questionnaire; 95%CI, confidence interval of 95%. Sample size=40. Spearman's coefficient (Rho) was used for statistics, with confidence interval of 95%. Only coefficients of positive associations are demonstrated. α=0.05.
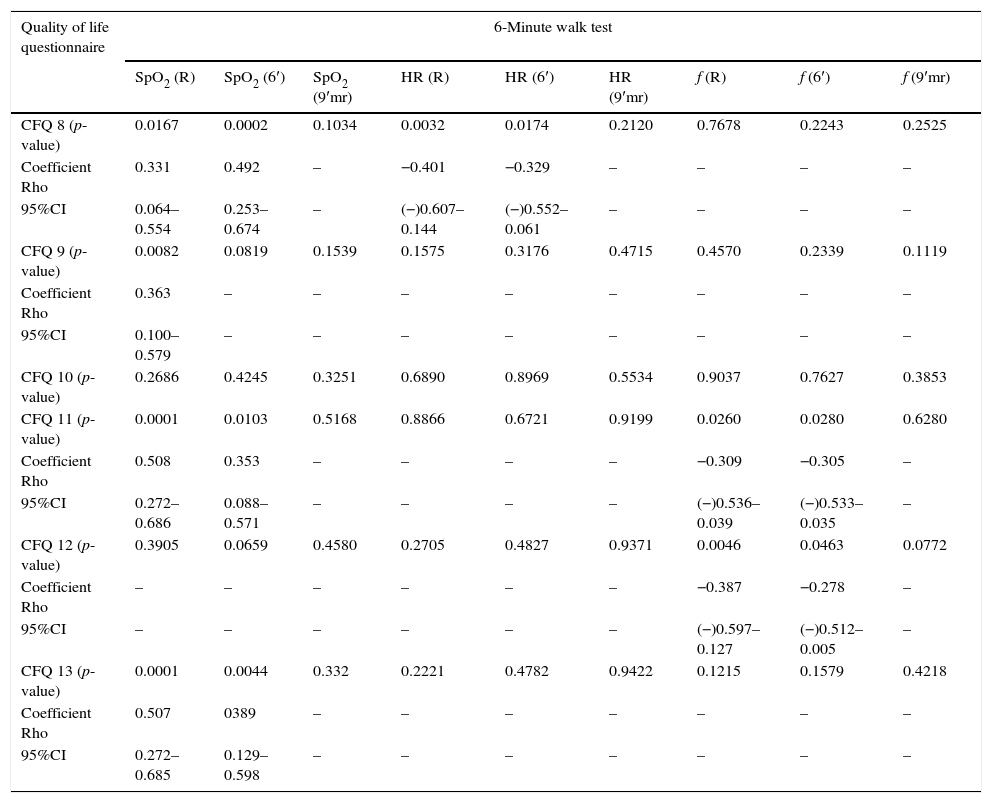
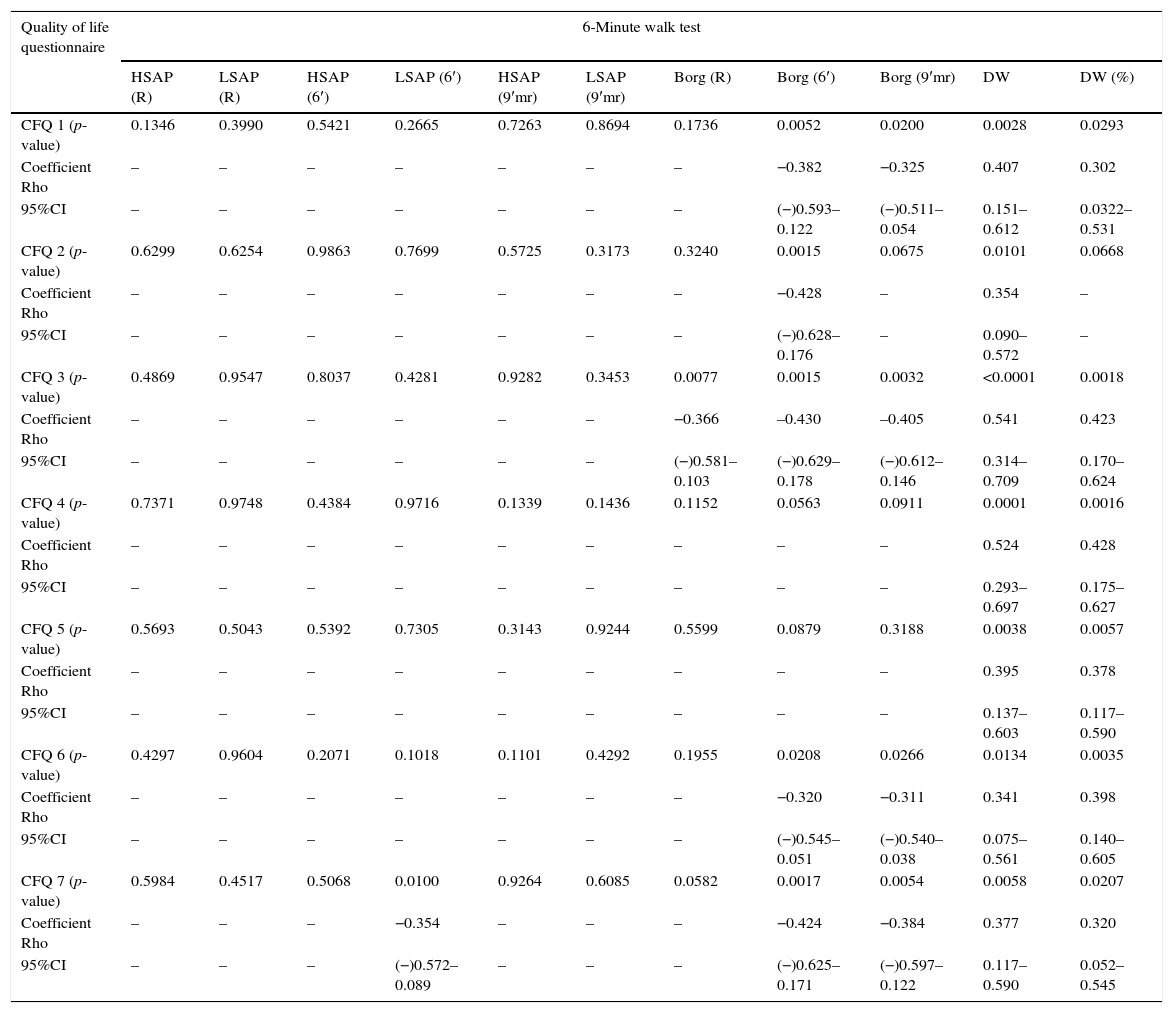
The correlation between the CFQ and the data obtained in the 6MWT of CF patients is shown in Tables 2A–3B.
Correlation between values of quality of life questionnaire and 6-minute walk test (SpO2, heart rate and inspiratory frequency) in patients with cystic fibrosis (Part I).
| Quality of life questionnaire | 6-Minute walk test | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| SpO2 (R) | SpO2 (6′) | SpO2 (9′mr) | HR (R) | HR (6′) | HR (9′mr) | f (R) | f (6′) | f (9′mr) | |
| CFQ 1 (p-value) | <0.0001 | 0.0004 | 0.1640 | 0.5220 | 0.7000 | 0.8879 | 0.1109 | 0.0304 | 0.2436 |
| Coefficient Rho | 0.583 | 0.473 | – | – | – | – | – | −0.301 | – |
| 95%CI | 0.369–0.739 | 0.229–0.660 | – | – | – | – | – | (−)0.530–0.030 | – |
| CFQ 2 (p-value) | 0.0096 | 0.0592 | 0.7858 | 0.0019 | 0.5240 | 0.3471 | 0.3880 | 0.0702 | 0.7829 |
| Coefficient Rho | 0.356 | – | – | −0.420 | – | – | – | – | – |
| 95%CI | 0.092–0.573 | – | – | (−)0.622–0.166 | – | – | – | – | – |
| CFQ 3 (p-value) | <0.0001 | 0.0005 | 0.0424 | 0.6392 | 0.7599 | 0.5048 | 0.2010 | 0.2584 | 0.4316 |
| Coefficient Rho | 0.566 | 0.467 | 0.285 | – | – | – | – | – | – |
| 95%CI | 0.346–0.726 | 0.222–0.656 | 0.011–0.520 | – | – | – | – | – | – |
| CFQ 4 (p-value) | 0.0008 | 0.0085 | 0.5322 | 0.2710 | 0.8988 | 0.6509 | 0.2029 | 0.4187 | 0.7994 |
| Coefficient Rho | 0.449 | 0.361 | – | – | – | – | – | – | – |
| 95%CI | 0.201–0.643 | 0.098–0.577 | – | – | – | – | – | – | – |
| CFQ 5 (p-value) | 0.2555 | 0.7440 | 0.4789 | 0.0383 | 0.9323 | 0.6584 | 0.8004 | 0.5808 | 0.4722 |
| Coefficient Rho | – | – | – | −0.288 | – | – | – | – | – |
| 95%CI | – | – | – | (−)0.520–0.017 | – | – | – | – | – |
| CFQ 6 (p-value) | 0.0431 | 0.2434 | 0.6180 | 0.7901 | 0.6996 | 0.8799 | 0.5434 | 0.3153 | 0.3542 |
| Coefficient Rho | 0.282 | – | – | – | – | – | – | – | – |
| 95%CI | 0.009–0.515 | – | – | – | – | – | – | – | – |
| CFQ 7 (p-value) | 0.0016 | 0.0199 | 0.0792 | 0.7472 | 0.5632 | 0.7588 | 0.2182 | 0.0357 | 0.0080 |
| Coefficient Rho | 0.426 | 0.322 | – | – | – | – | – | −0.292 | −0.368 |
| 95%CI | 0.174–0.626 | 0.054–0.547 | – | – | – | – | – | (−)0.523–0.021 | (−)0.584–0.102 |
CFQ, quality of life questionnaire for cystic fibrosis; 95%CI, confidence interval of 95%; SpO2, peripheral oxygen saturation of hemoglobin; HR, heart rate; f, inspiratory frequency; R, rest; 6′, 6-min period of walk test; 9′mr, 9-min rest after the end of the walk test. Sample size=52 (except for 9′mr=51 patients). Spearman's coefficient (Rho) was used for statistics with confidence interval of 95%. Only coefficients of positive associations are demonstrated. α=0.05.
Correlation between values of quality of life questionnaire and 6-minute walk test (SpO2, heart rate and inspiratory frequency) in patients with cystic fibrosis (Part II).
| Quality of life questionnaire | 6-Minute walk test | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| SpO2 (R) | SpO2 (6′) | SpO2 (9′mr) | HR (R) | HR (6′) | HR (9′mr) | f (R) | f (6′) | f (9′mr) | |
| CFQ 8 (p-value) | 0.0167 | 0.0002 | 0.1034 | 0.0032 | 0.0174 | 0.2120 | 0.7678 | 0.2243 | 0.2525 |
| Coefficient Rho | 0.331 | 0.492 | – | −0.401 | −0.329 | – | – | – | – |
| 95%CI | 0.064–0.554 | 0.253–0.674 | – | (−)0.607–0.144 | (−)0.552–0.061 | – | – | – | – |
| CFQ 9 (p-value) | 0.0082 | 0.0819 | 0.1539 | 0.1575 | 0.3176 | 0.4715 | 0.4570 | 0.2339 | 0.1119 |
| Coefficient Rho | 0.363 | – | – | – | – | – | – | – | – |
| 95%CI | 0.100–0.579 | – | – | – | – | – | – | – | – |
| CFQ 10 (p-value) | 0.2686 | 0.4245 | 0.3251 | 0.6890 | 0.8969 | 0.5534 | 0.9037 | 0.7627 | 0.3853 |
| CFQ 11 (p-value) | 0.0001 | 0.0103 | 0.5168 | 0.8866 | 0.6721 | 0.9199 | 0.0260 | 0.0280 | 0.6280 |
| Coefficient Rho | 0.508 | 0.353 | – | – | – | – | −0.309 | −0.305 | – |
| 95%CI | 0.272–0.686 | 0.088–0.571 | – | – | – | – | (−)0.536–0.039 | (−)0.533–0.035 | – |
| CFQ 12 (p-value) | 0.3905 | 0.0659 | 0.4580 | 0.2705 | 0.4827 | 0.9371 | 0.0046 | 0.0463 | 0.0772 |
| Coefficient Rho | – | – | – | – | – | – | −0.387 | −0.278 | – |
| 95%CI | – | – | – | – | – | – | (−)0.597–0.127 | (−)0.512–0.005 | – |
| CFQ 13 (p-value) | 0.0001 | 0.0044 | 0.332 | 0.2221 | 0.4782 | 0.9422 | 0.1215 | 0.1579 | 0.4218 |
| Coefficient Rho | 0.507 | 0389 | – | – | – | – | – | – | – |
| 95%CI | 0.272–0.685 | 0.129–0.598 | – | – | – | – | – | – | – |
CFQ, quality of life questionnaire for cystic fibrosis; 95%CI, confidence interval of 95%; SpO2, peripheral oxygen saturation of hemoglobin; HR, heart rate; f, inspiratory frequency; R, rest; 6′, 6-min period of walk test; 9′mr, 9-min rest after the end of the walk test. Sample size=52 (except for 9′mr=51 patients). Spearman's coefficient (Rho) was used for statistics with confidence interval of 95%. Only coefficients of positive associations are demonstrated shown. α=0.05.
Correlation between values of quality of life questionnaire and 6-minute walk test (systemic arterial pressure, Borg scale, and waking distance) in patients with cystic fibrosis (Part I).
| Quality of life questionnaire | 6-Minute walk test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HSAP (R) | LSAP (R) | HSAP (6′) | LSAP (6′) | HSAP (9′mr) | LSAP (9′mr) | Borg (R) | Borg (6′) | Borg (9′mr) | DW | DW (%) | |
| CFQ 1 (p-value) | 0.1346 | 0.3990 | 0.5421 | 0.2665 | 0.7263 | 0.8694 | 0.1736 | 0.0052 | 0.0200 | 0.0028 | 0.0293 |
| Coefficient Rho | – | – | – | – | – | – | – | −0.382 | −0.325 | 0.407 | 0.302 |
| 95%CI | – | – | – | – | – | – | – | (−)0.593–0.122 | (−)0.511–0.054 | 0.151–0.612 | 0.0322–0.531 |
| CFQ 2 (p-value) | 0.6299 | 0.6254 | 0.9863 | 0.7699 | 0.5725 | 0.3173 | 0.3240 | 0.0015 | 0.0675 | 0.0101 | 0.0668 |
| Coefficient Rho | – | – | – | – | – | – | – | −0.428 | – | 0.354 | – |
| 95%CI | – | – | – | – | – | – | – | (−)0.628–0.176 | – | 0.090–0.572 | – |
| CFQ 3 (p-value) | 0.4869 | 0.9547 | 0.8037 | 0.4281 | 0.9282 | 0.3453 | 0.0077 | 0.0015 | 0.0032 | <0.0001 | 0.0018 |
| Coefficient Rho | – | – | – | – | – | – | −0.366 | –0.430 | –0.405 | 0.541 | 0.423 |
| 95%CI | – | – | – | – | – | – | (−)0.581–0.103 | (−)0.629–0.178 | (−)0.612–0.146 | 0.314–0.709 | 0.170–0.624 |
| CFQ 4 (p-value) | 0.7371 | 0.9748 | 0.4384 | 0.9716 | 0.1339 | 0.1436 | 0.1152 | 0.0563 | 0.0911 | 0.0001 | 0.0016 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.524 | 0.428 |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.293–0.697 | 0.175–0.627 |
| CFQ 5 (p-value) | 0.5693 | 0.5043 | 0.5392 | 0.7305 | 0.3143 | 0.9244 | 0.5599 | 0.0879 | 0.3188 | 0.0038 | 0.0057 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.395 | 0.378 |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.137–0.603 | 0.117–0.590 |
| CFQ 6 (p-value) | 0.4297 | 0.9604 | 0.2071 | 0.1018 | 0.1101 | 0.4292 | 0.1955 | 0.0208 | 0.0266 | 0.0134 | 0.0035 |
| Coefficient Rho | – | – | – | – | – | – | – | −0.320 | −0.311 | 0.341 | 0.398 |
| 95%CI | – | – | – | – | – | – | – | (−)0.545–0.051 | (−)0.540–0.038 | 0.075–0.561 | 0.140–0.605 |
| CFQ 7 (p-value) | 0.5984 | 0.4517 | 0.5068 | 0.0100 | 0.9264 | 0.6085 | 0.0582 | 0.0017 | 0.0054 | 0.0058 | 0.0207 |
| Coefficient Rho | – | – | – | −0.354 | – | – | – | −0.424 | −0.384 | 0.377 | 0.320 |
| 95%CI | – | – | – | (−)0.572–0.089 | – | – | – | (−)0.625–0.171 | (−)0.597–0.122 | 0.117–0.590 | 0.052–0.545 |
CFQ, quality of life questionnaire for cystic fibrosis; 95%CI, confidence interval of 95%; HSAP, high systemic arterial pressure; LSAP, low systemic arterial pressure; DW, distance walked; R, rest; 6′, 6-min period of walk test; 9′mr, 9-min rest after the end of the walk test. Sample size=52 (except for 9′mr=51 patients). Spearman's coefficient (Rho) was used for statistics with confidence interval of 95%. Only coefficients of positive associations are demonstrated. α=0.05.
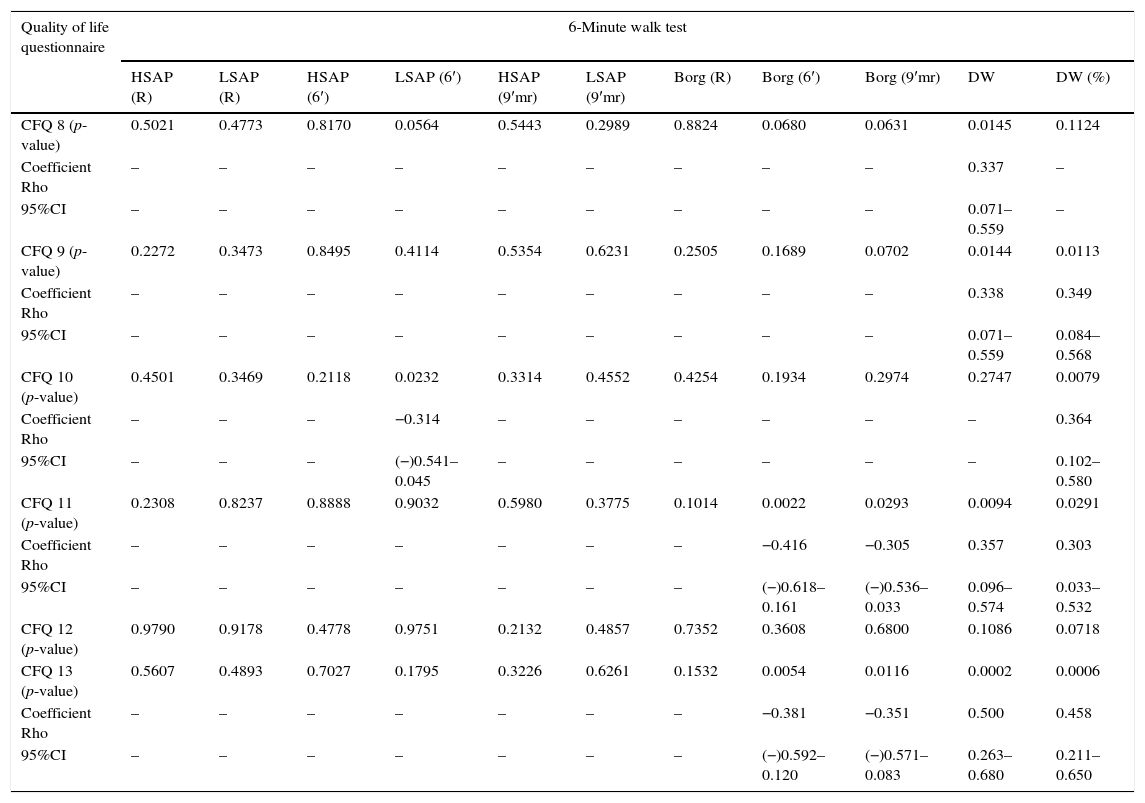
Correlation between values of quality of life questionnaire and 6-minute walk test (systemic arterial pressure, Borg scale, and waking distance) in patients with cystic fibrosis (Part II).
| Quality of life questionnaire | 6-Minute walk test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HSAP (R) | LSAP (R) | HSAP (6′) | LSAP (6′) | HSAP (9′mr) | LSAP (9′mr) | Borg (R) | Borg (6′) | Borg (9′mr) | DW | DW (%) | |
| CFQ 8 (p-value) | 0.5021 | 0.4773 | 0.8170 | 0.0564 | 0.5443 | 0.2989 | 0.8824 | 0.0680 | 0.0631 | 0.0145 | 0.1124 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.337 | – |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.071–0.559 | – |
| CFQ 9 (p-value) | 0.2272 | 0.3473 | 0.8495 | 0.4114 | 0.5354 | 0.6231 | 0.2505 | 0.1689 | 0.0702 | 0.0144 | 0.0113 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.338 | 0.349 |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.071–0.559 | 0.084–0.568 |
| CFQ 10 (p-value) | 0.4501 | 0.3469 | 0.2118 | 0.0232 | 0.3314 | 0.4552 | 0.4254 | 0.1934 | 0.2974 | 0.2747 | 0.0079 |
| Coefficient Rho | – | – | – | −0.314 | – | – | – | – | – | – | 0.364 |
| 95%CI | – | – | – | (−)0.541–0.045 | – | – | – | – | – | – | 0.102–0.580 |
| CFQ 11 (p-value) | 0.2308 | 0.8237 | 0.8888 | 0.9032 | 0.5980 | 0.3775 | 0.1014 | 0.0022 | 0.0293 | 0.0094 | 0.0291 |
| Coefficient Rho | – | – | – | – | – | – | – | −0.416 | −0.305 | 0.357 | 0.303 |
| 95%CI | – | – | – | – | – | – | – | (−)0.618–0.161 | (−)0.536–0.033 | 0.096–0.574 | 0.033–0.532 |
| CFQ 12 (p-value) | 0.9790 | 0.9178 | 0.4778 | 0.9751 | 0.2132 | 0.4857 | 0.7352 | 0.3608 | 0.6800 | 0.1086 | 0.0718 |
| CFQ 13 (p-value) | 0.5607 | 0.4893 | 0.7027 | 0.1795 | 0.3226 | 0.6261 | 0.1532 | 0.0054 | 0.0116 | 0.0002 | 0.0006 |
| Coefficient Rho | – | – | – | – | – | – | – | −0.381 | −0.351 | 0.500 | 0.458 |
| 95%CI | – | – | – | – | – | – | – | (−)0.592–0.120 | (−)0.571–0.083 | 0.263–0.680 | 0.211–0.650 |
CFQ, quality of life questionnaire for cystic fibrosis; 95%CI, confidence interval of 95%; HSAP, high systemic arterial pressure; LSAP, low systemic arterial pressure; DW, distance walked; R, rest; 6′, 6-min period of walk test; 9′mr, 9-min rest after the end of the walk test. Sample size=52 (except for 9′mr=51 patients). Spearman's coefficient (Rho) was used for statistics with confidence interval of 95%. Only coefficients of positive associations are demonstrated. α=0.05.
The correlation between SSQ and the data obtained in the 6MWT of CF patients is shown in Tables 4A–4C.
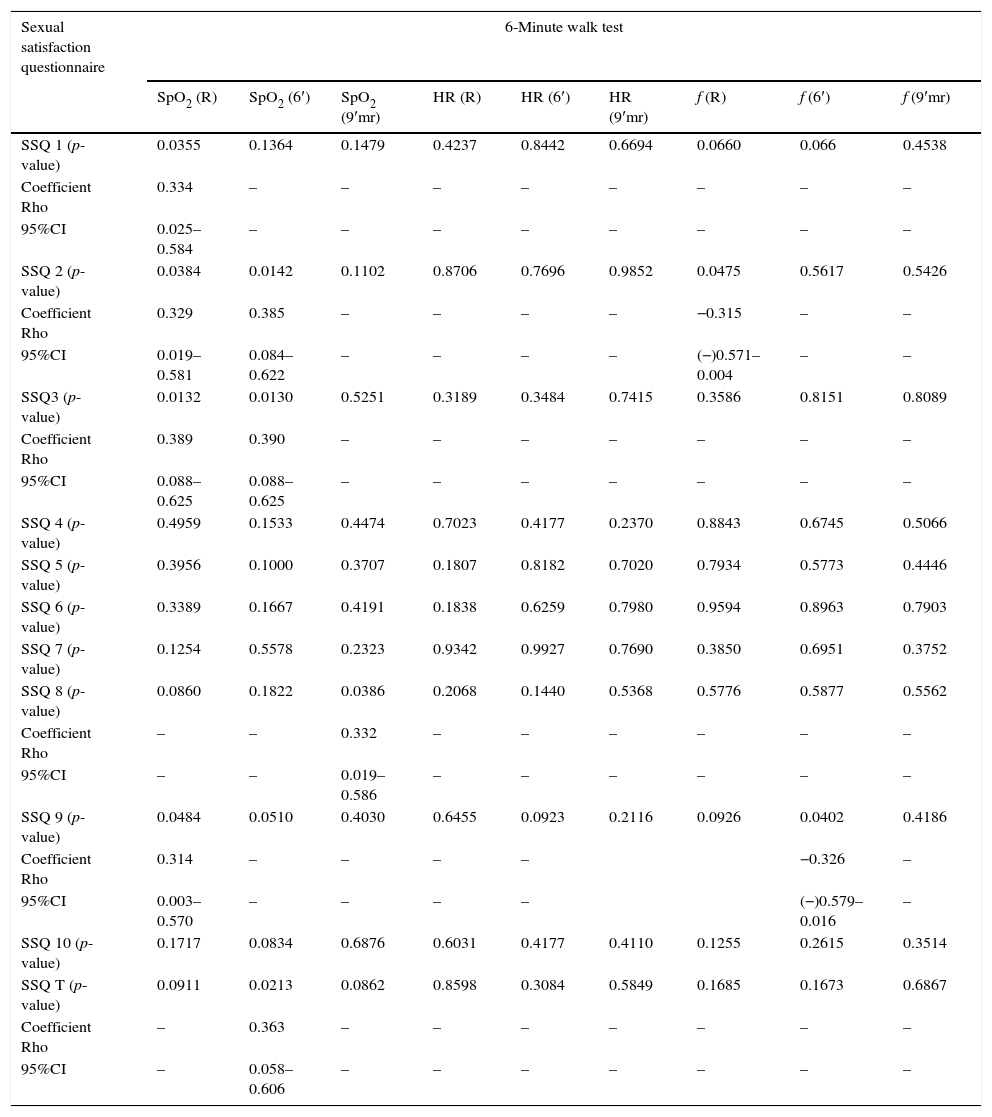
Correlation between values of sexual satisfaction questionnaire and the 6-minute walk test (SpO2, heart rate and inspiratory frequency) in patients with cystic fibrosis (Part I).
| Sexual satisfaction questionnaire | 6-Minute walk test | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| SpO2 (R) | SpO2 (6′) | SpO2 (9′mr) | HR (R) | HR (6′) | HR (9′mr) | f (R) | f (6′) | f (9′mr) | |
| SSQ 1 (p-value) | 0.0355 | 0.1364 | 0.1479 | 0.4237 | 0.8442 | 0.6694 | 0.0660 | 0.066 | 0.4538 |
| Coefficient Rho | 0.334 | – | – | – | – | – | – | – | – |
| 95%CI | 0.025–0.584 | – | – | – | – | – | – | – | – |
| SSQ 2 (p-value) | 0.0384 | 0.0142 | 0.1102 | 0.8706 | 0.7696 | 0.9852 | 0.0475 | 0.5617 | 0.5426 |
| Coefficient Rho | 0.329 | 0.385 | – | – | – | – | −0.315 | – | – |
| 95%CI | 0.019–0.581 | 0.084–0.622 | – | – | – | – | (−)0.571–0.004 | – | – |
| SSQ3 (p-value) | 0.0132 | 0.0130 | 0.5251 | 0.3189 | 0.3484 | 0.7415 | 0.3586 | 0.8151 | 0.8089 |
| Coefficient Rho | 0.389 | 0.390 | – | – | – | – | – | – | – |
| 95%CI | 0.088–0.625 | 0.088–0.625 | – | – | – | – | – | – | – |
| SSQ 4 (p-value) | 0.4959 | 0.1533 | 0.4474 | 0.7023 | 0.4177 | 0.2370 | 0.8843 | 0.6745 | 0.5066 |
| SSQ 5 (p-value) | 0.3956 | 0.1000 | 0.3707 | 0.1807 | 0.8182 | 0.7020 | 0.7934 | 0.5773 | 0.4446 |
| SSQ 6 (p-value) | 0.3389 | 0.1667 | 0.4191 | 0.1838 | 0.6259 | 0.7980 | 0.9594 | 0.8963 | 0.7903 |
| SSQ 7 (p-value) | 0.1254 | 0.5578 | 0.2323 | 0.9342 | 0.9927 | 0.7690 | 0.3850 | 0.6951 | 0.3752 |
| SSQ 8 (p-value) | 0.0860 | 0.1822 | 0.0386 | 0.2068 | 0.1440 | 0.5368 | 0.5776 | 0.5877 | 0.5562 |
| Coefficient Rho | – | – | 0.332 | – | – | – | – | – | – |
| 95%CI | – | – | 0.019–0.586 | – | – | – | – | – | – |
| SSQ 9 (p-value) | 0.0484 | 0.0510 | 0.4030 | 0.6455 | 0.0923 | 0.2116 | 0.0926 | 0.0402 | 0.4186 |
| Coefficient Rho | 0.314 | – | – | – | – | −0.326 | – | ||
| 95%CI | 0.003–0.570 | – | – | – | – | (−)0.579–0.016 | – | ||
| SSQ 10 (p-value) | 0.1717 | 0.0834 | 0.6876 | 0.6031 | 0.4177 | 0.4110 | 0.1255 | 0.2615 | 0.3514 |
| SSQ T (p-value) | 0.0911 | 0.0213 | 0.0862 | 0.8598 | 0.3084 | 0.5849 | 0.1685 | 0.1673 | 0.6867 |
| Coefficient Rho | – | 0.363 | – | – | – | – | – | – | – |
| 95%CI | – | 0.058–0.606 | – | – | – | – | – | – | – |
SSQ, sexual satisfaction questionnaire; SSQT, sexual satisfaction questionnaire-total; 95%CI, confidence interval of 95%; SpO2, peripheral oxygen saturation of hemoglobin; HR, heart rate; f, inspiratory frequency; R, rest; 6′, 6-min period of walk test; 9′mr, 9-min rest after the end of the walk test. Sample size=40. Spearman's coefficient (Rho) was used for statistics with confidence interval of 95%. Only coefficients of positive associations are demonstrated. SSQ data which showed no association with any of the markers of the walk test are demonstrated with p-value only. α=0.05.
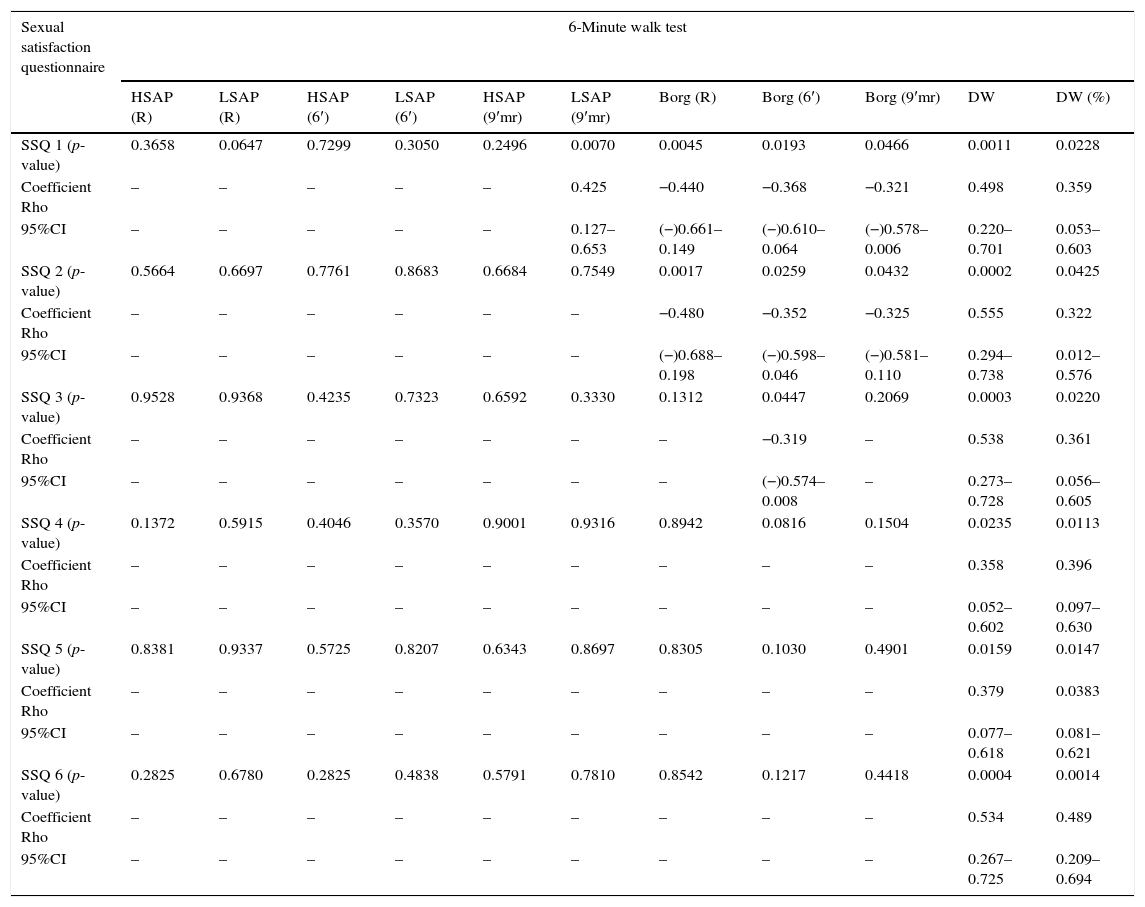
Correlation between values of quality of life questionnaire and the 6-minute walk test (systemic arterial pressure, Borg scale and distance walked) in patients with cystic fibrosis (Part II).
| Sexual satisfaction questionnaire | 6-Minute walk test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HSAP (R) | LSAP (R) | HSAP (6′) | LSAP (6′) | HSAP (9′mr) | LSAP (9′mr) | Borg (R) | Borg (6′) | Borg (9′mr) | DW | DW (%) | |
| SSQ 1 (p-value) | 0.3658 | 0.0647 | 0.7299 | 0.3050 | 0.2496 | 0.0070 | 0.0045 | 0.0193 | 0.0466 | 0.0011 | 0.0228 |
| Coefficient Rho | – | – | – | – | – | 0.425 | −0.440 | −0.368 | −0.321 | 0.498 | 0.359 |
| 95%CI | – | – | – | – | – | 0.127–0.653 | (−)0.661–0.149 | (−)0.610–0.064 | (−)0.578–0.006 | 0.220–0.701 | 0.053–0.603 |
| SSQ 2 (p-value) | 0.5664 | 0.6697 | 0.7761 | 0.8683 | 0.6684 | 0.7549 | 0.0017 | 0.0259 | 0.0432 | 0.0002 | 0.0425 |
| Coefficient Rho | – | – | – | – | – | – | −0.480 | −0.352 | −0.325 | 0.555 | 0.322 |
| 95%CI | – | – | – | – | – | – | (−)0.688–0.198 | (−)0.598–0.046 | (−)0.581–0.110 | 0.294–0.738 | 0.012–0.576 |
| SSQ 3 (p-value) | 0.9528 | 0.9368 | 0.4235 | 0.7323 | 0.6592 | 0.3330 | 0.1312 | 0.0447 | 0.2069 | 0.0003 | 0.0220 |
| Coefficient Rho | – | – | – | – | – | – | – | −0.319 | – | 0.538 | 0.361 |
| 95%CI | – | – | – | – | – | – | – | (−)0.574–0.008 | – | 0.273–0.728 | 0.056–0.605 |
| SSQ 4 (p-value) | 0.1372 | 0.5915 | 0.4046 | 0.3570 | 0.9001 | 0.9316 | 0.8942 | 0.0816 | 0.1504 | 0.0235 | 0.0113 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.358 | 0.396 |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.052–0.602 | 0.097–0.630 |
| SSQ 5 (p-value) | 0.8381 | 0.9337 | 0.5725 | 0.8207 | 0.6343 | 0.8697 | 0.8305 | 0.1030 | 0.4901 | 0.0159 | 0.0147 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.379 | 0.0383 |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.077–0.618 | 0.081–0.621 |
| SSQ 6 (p-value) | 0.2825 | 0.6780 | 0.2825 | 0.4838 | 0.5791 | 0.7810 | 0.8542 | 0.1217 | 0.4418 | 0.0004 | 0.0014 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.534 | 0.489 |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.267–0.725 | 0.209–0.694 |
SSQ, sexual satisfaction questionnaire; 95%CI, confidence interval of 95%; HSAP, high systemic arterial pressure; LSAP, low systemic arterial pressure; HR, heart rate; DW, distance walked; R, rest; 6′, 6-min period of walk test; 9′mr, 9-min rest after the end of the walk test. Sample size=40. Spearman's coefficient (Rho) was used for statistics with confidence interval of 95%. Only coefficient of positive associations are shown α=0.05.
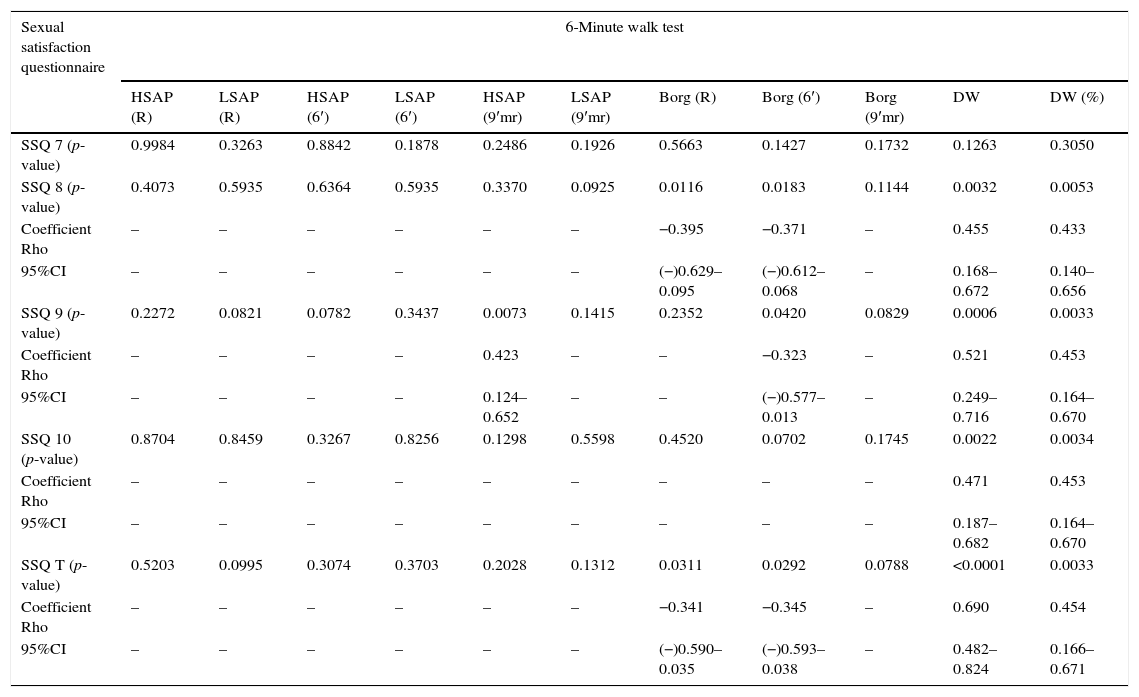
Correlation between values of quality of life questionnaire and the 6-minute walk test (systemic arterial pressure, Borg scale and distance walked) in patients with cystic fibrosis (Part III).
| Sexual satisfaction questionnaire | 6-Minute walk test | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| HSAP (R) | LSAP (R) | HSAP (6′) | LSAP (6′) | HSAP (9′mr) | LSAP (9′mr) | Borg (R) | Borg (6′) | Borg (9′mr) | DW | DW (%) | |
| SSQ 7 (p-value) | 0.9984 | 0.3263 | 0.8842 | 0.1878 | 0.2486 | 0.1926 | 0.5663 | 0.1427 | 0.1732 | 0.1263 | 0.3050 |
| SSQ 8 (p-value) | 0.4073 | 0.5935 | 0.6364 | 0.5935 | 0.3370 | 0.0925 | 0.0116 | 0.0183 | 0.1144 | 0.0032 | 0.0053 |
| Coefficient Rho | – | – | – | – | – | – | −0.395 | −0.371 | – | 0.455 | 0.433 |
| 95%CI | – | – | – | – | – | – | (−)0.629–0.095 | (−)0.612–0.068 | – | 0.168–0.672 | 0.140–0.656 |
| SSQ 9 (p-value) | 0.2272 | 0.0821 | 0.0782 | 0.3437 | 0.0073 | 0.1415 | 0.2352 | 0.0420 | 0.0829 | 0.0006 | 0.0033 |
| Coefficient Rho | – | – | – | – | 0.423 | – | – | −0.323 | – | 0.521 | 0.453 |
| 95%CI | – | – | – | – | 0.124–0.652 | – | – | (−)0.577–0.013 | – | 0.249–0.716 | 0.164–0.670 |
| SSQ 10 (p-value) | 0.8704 | 0.8459 | 0.3267 | 0.8256 | 0.1298 | 0.5598 | 0.4520 | 0.0702 | 0.1745 | 0.0022 | 0.0034 |
| Coefficient Rho | – | – | – | – | – | – | – | – | – | 0.471 | 0.453 |
| 95%CI | – | – | – | – | – | – | – | – | – | 0.187–0.682 | 0.164–0.670 |
| SSQ T (p-value) | 0.5203 | 0.0995 | 0.3074 | 0.3703 | 0.2028 | 0.1312 | 0.0311 | 0.0292 | 0.0788 | <0.0001 | 0.0033 |
| Coefficient Rho | – | – | – | – | – | – | −0.341 | −0.345 | – | 0.690 | 0.454 |
| 95%CI | – | – | – | – | – | – | (−)0.590–0.035 | (−)0.593–0.038 | – | 0.482–0.824 | 0.166–0.671 |
SSQ, sexual satisfaction questionnaire; SSQT, sexual satisfaction questionnaire-total; 95%CI, confidence interval of 95%; HSAP, high systemic arterial pressure; LSAP, low systemic arterial pressure; DW, distance walked; R, rest; 6′, 6-min period of walk test; 9′mr, 9-min rest after the end of the walk test. Sample size=40. Spearman's coefficient (Rho) was used for statistics with confidence interval of 95%. Only coefficients of positive associations are demonstrated SSQ data which showed no association with any of the markers of the walk test are demonstrated with p-value. α=0.05.
The association of gender and data of SSQ and CFQ, and the markers assessed in 6MWT are shown in Online Resources 3 and 4. The p-value for associations with the gender of CF patient is presented in Online Resource 5.
DiscussionTo the best of our knowledge, this is the first study to correlate physical performance, QOL and SS and, using 6MWT, CFQ and SSQ, simultaneously, in CF adult patients. Our study found correlations among all tests.
CFQ is a disease-specific qualify of life measure for CF patients; however, it does not assess sexuality. Therefore, the SSQ should be introduced in order to evaluate SS. Although SSQ is not exclusively tailored to CF patients, it can be introduced as a routine follow-up of CF patients, as life expectancy and the number of sexually active patients have considerably increased worldwide. This can only reaffirm the importance of including SS for the assessment of QOL in further researches.
CF patients may have problems engaging in sexual activity and later building a stable relationship with a partner. The QOL of CF patients will strongly depend on how they cope with the disease.12 Mutual actions between QOL and SS could be observed. Despite the limitations caused by CF, studies report that adult patients expected to establish a sexual relationship and experience maternity and paternity.4,13 However, as the disease progresses, severity will continuously increase, followed by decline of QOL and SS.
It is of utmost importance that the probability of pregnancy and all risks and benefits for the CF patient be explained, in the event of expectations about becoming a parent. This includes clarifying the limitations of the disease for both sexes: (i) obstruction of the vas deferens and azoospermia; (ii) difficulty in getting pregnant due to physiological changes in the uterus; (iii) higher risk of complications during pregnancy; (iv) increased clinical severity after pregnancy; and (v) higher risk of CF the offspring.14–16
In CF, sexual dissatisfaction may occur due to physical and psychological factors. Physical factors are caused by progressive deterioration of the function of various organs, such as lungs, liver, pancreas, bones, muscles and joints, which require continuous treatment throughout the patient's lifetime. Daily treatment includes administration of oral or inhaled medications, physiotherapy, follow-up visits to the referral centers and hospitals, and periodic examinations. Also, in case of pulmonary exacerbations, patients will require hospitalization, which will pose a negative impact on physical and emotional well-being. This study showed a correlation between SS and QOL, where best scores in QOL were linked to better scores in SS.
In the CFQ, the domains 1 (physical role), 3 (vitality), 6 (body image), 9 (health perceptions) and 11 (respiratory symptoms) had positive correlation with SSQ for answers about sex drive, self-confidence, willingness to initiate sexual activity, foreplay and ability to reach orgasm. QOL and SS are associated with the individual's perception of health, which will determine the relationship quality with the partner. The better the individual feels, the greater is the ability to perform his activities (physical and social) and to accept sexual relationships.17
Emotional changes, including depression, are common issues that CF patients face. These changes affect adherence to treatment, social life, and QOL and SS, especially among adults.18–21 Psychological aspects have been evaluated in qualitative studies and studies associated with QOL, as they influence almost all aspects of the disease and may affect directly or indirectly SS.22
Questions about sexuality and about how CF might affect patients’ sexual health are rarely discussed with the doctor. During the CF follow up, doctors tend to focus on the treatment of the disease, and not on the emotional factors, such as fears, uncertainties, insecurities related to sexuality.15,23 In this context, the role of a psychologist and the support of an interdisciplinary team of professionals are of utmost importance in the CF reference centers.
This study also approached the patient's physical evaluation conducted by 6MWT. There was a correlation between QOL and 6MWT as markers of progression of lung disease, as well as between SpO2 and distance walked. Higher values of CFQ had a positive correlation. This finding was confirmed by a no correlation between the Borg scale and CFQ before 6MWT. However, there was a negative correlation during and after the exercise session. Thus, patients with better QOL had lower values on the Borg scale. This is possibly associated with better performance and less fatigue during the 6MWT.
Numerous studies show that physical activity is important for QOL. Aerobic exercise and muscle strength training improve bronchial tree patency, avoid progressive decline in lung function, improve muscle mass and resistance to exercise, promote bone growth, boost self-esteem, and may have an impact on QOL24–26 and, eventually, on sexuality.
The SS was negatively correlated with the Borg scale in the three time periods, mainly at rest and during the 6-min period of activity. Physical activity is an important marker of satisfactory physical development of patients and acts on the improvement of SS.24–26
The distance walked showed positive correlation with all SSQ questions, except for question 7. This may be the result of better physical condition, and consequently, better sexual activity, which confirms a relationship between physical performance and SS.
The delay in diagnosing the disease was higher among men and the age of inclusion in the study was higher in women. Males have less inflammation during puberty, which allowed delayed diagnosis of the disease. Female age was higher, possibly associated with minor environmental and genetic factors, which should be further investigated.
At first, we believed that males would have greater difficulty obtaining SS. Such belief was based on tiredness after sex and higher probability of male infertility (∼95%).27,28 It could create internal and external conflicts, which might negatively affect SS. However, in our study, males obtained higher score in the SSQ. The same occurred with the scores for distance walked in the 6MWT and emotional fitness in CFQ.
As reported in the literature, women tend to show greater concern about the disease and lower values in QOL.29 Another aspect to be considered in the analysis of QOL and SS is that women with CF usually have worse clinical outcomes.30
Limitations to this study included: (i) not all patients included in this study had initiated sexual activity and/or had been sexually active in the past 6 months; (ii) two invited patients refused to participate in this study; (iii) SSQ is not as specific for CF as the CFQ; (iv) the evaluation of questions 4 and 7 of SSQ has unpaired content between the QSF and QSM. However, these were the questions, which demonstrate lower correlation.
In conclusion, adult CF patients present correlation between 6MWT, QOL and SS. We believe that sexuality should be evaluated in QOL surveys, as well as the assessment of physical performance.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
Confidentiality of dataThe authors declare that they have followed the protocols of their work centre on the publication of patient data.
Right to privacy and informed consentThe authors must have obtained the informed consent of the patients and/or subjects mentioned in the article. The author for correspondence must be in possession of this document.
FundingFinancial support from the following institutions: KCAA: Coordenação de Aperfeiçoamento de Pessoal de Nível Superior Capes#01-P-03492/2014; FALM: Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) for sponsoring the researches #2011/12939-4, #2011/18845-1, #2015/12183-8 and #2015/12858-5; and Fundo de Apoio à Pesquisa, ao Ensino e à Extensão da Universidade Estadual de Campinas for sponsoring the research #0648/2015. JDR: Fapesp for sponsoring the researches #2011/18845-1, #2012/05458-2 and #2015/12183-8.
Author contributionsKKAA/FALM has made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; drafted the submitted article and revised it critically for important intellectual content and provided final approval of the version to be published; CCSG/IAP/MCP/AFR has made substantial contributions to conception, design and acquisition of data; JDR has drafted the submitted article and revised it critically for important intellectual content and provided final approval of the version to be published.
Conflicts of interestThe authors have no conflicts of interest to declare.
The group of cystic fibrosis: Maria Ângela Gonçalves de Oliveira Ribeiro, Carmen Sílvia Bertuzzo, Carlos Emilio Levy, Roberto José Negrão Nogueira, Eulália Sakano, Andressa Oliveira Peixoto, Gabriel Hessel and Adyléia Dalbo Contrera Toro.
Carmita Abdo to allow the use of the test about sexuality. Tatiana Rozov, who provided us with the quality of life test and gave us the permission to use it.
All patients who participated in this study.
The following are the supplementary data to this article:


